REALITY #3: WAKE ME UP WHEN SEPTEMBER 2016 ENDS
THE TAKE HOME: This blog is a written account of a two hour live webinar I gave to members in Sept of 2016. Most of them felt this information was so important that they voted 89% to publish this info for public consumption. I will remind you all these members paid for this content so when you read it I hope you all thank a www.jackkruse.com member. Jamie Ward was the member who originally suggested that I take the filmed webinar and make it a blog for public consumption. It took me a while to write it all down from the filmed recording I did in August of 2016. The point of this webinar is to show you the sun is not bad for health bu the light man has created for modern man to live under is toxic for mitochondria and leads to the diseases that modern healthcare blames the sun for. I use ocular melanoma to make the point.
The modern belief is that UV light, alone, causes melanoma and melanogenesis by the healthcare paradigm. The reality is that this is a belief, but is it well supported in the literature?
Today, 32% of Americans suffer from vitamin D3 insufficiency. Almost every modern human disease is linked to poor Vitamin D3 creation. There is far more risk to people from avoiding the sun and exposing themselves to artificial light (particularly violet and blue). “But what about melanoma?” critics cry. Did you know outdoor workers have a lower incidence of melanoma than indoor workers? Yes, melanoma incidence has risen 23 times from 1935-2012, but guess what other shifts happened from 1880 through today? Man began to gorge on an artificial light while burying the sun from their life. Today, we now have a population of people putting a blue light in their eyes and on their skin inside 24/7 now. From 1970 through 2009, age- and sex-adjusted incidence increased significantly over time (P<.001) from 7.9 to 60.0 per 100,000 person-years, with a 24-fold increase in women and a 4.5-fold increase in men. HYPERLINK
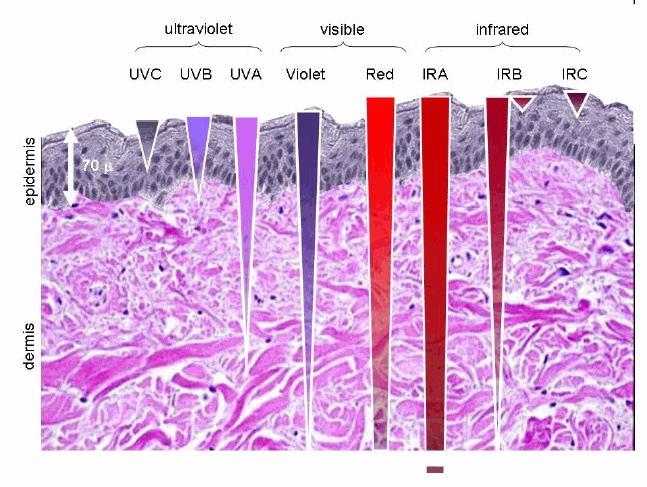
Corporate scientists created papers that allowed for clinicians to believe that UV light was always bad and this lead to the mass adoption of sunscreen. Sunscreen lowers Vitamin D3 in a massive fashion immediately because UV light makes D3 on the surface of skin and UV does not penetrate the skin deeply. Blue light, labeled violet below however does. Melanopsin is known to be present in the skin and subcutaneous fat.
In the last 100 years, the workforce in the USA has shifted from 75% outside to 75% inside (and that’s only up since 2000). If the sun is to blame, then how come vitamin D3 rates are at historic lows, while melanoma rates are 23 times higher?
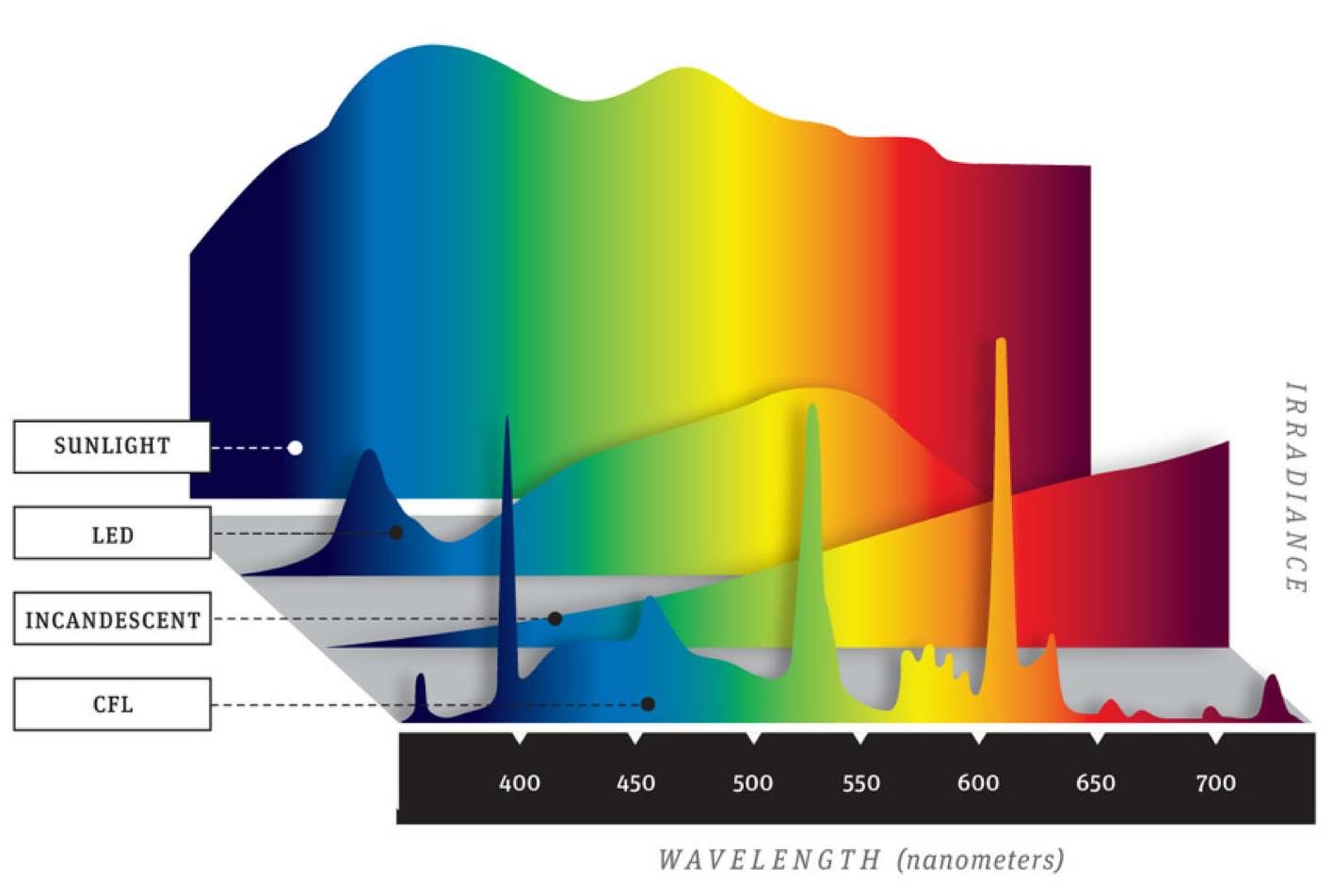
Visible light (400–700 nm) lies outside of the spectral range of what photobiologists define as deleterious radiation and as a result, few studies have studied the effects of a visible light range of wavelengths on the skin (250-3100nm). This oversight is important considering that during outdoors activities skin is exposed to the full solar spectrum, including visible light, and to multiple exposures at different times and doses. Its been established that the UV component of light from man-made sources can cause skin damage, few studies have examined the effects of non-UV solar full spectrum radiation on skin physiology in terms of inflammation and pigmentation. In fact, you might be shocked to know there is very limited information is available regarding the role of visible light on pigmentation. This is interesting because in the melanoma literature it is well documented that melanomas tend to be associated with origins in nevi on the skin.
Skin plays a role as a biological active barrier to the external environment including sun exposure and the presence of cutaneous hypothalamic-pituitary-adrenal axis (HPA) makes it an important peripheral neuroendocrine organ. The skin acts not only as a target for neuroendocrine signals but also a source of hormones and neurotransmitters, particularly the epidermis. As a result, biological responses for pigmentation formation do not necessarily share the same mechanism of action to environmental insults including different wavelengths of sun exposure. A single exposure of UVB can induce delayed pigment formation preceded by an erythema response. UVA (320–400 nm) can induce IPD (immediate pigment darkening) during the first minutes of exposure, which is transient form of pigmentation and fades away within few hours, or PPD (persistent pigment darkening) that appears within hours of higher doses of UVA exposure and persist up to several days or weeks. Both IPD and PPD, as well as erythema, has been shown to be induced in skin phototypes I and II by single UVA exposure and some studies in fair-skinned persons have also investigated the increase in pigmentation after multiple exposures of UVA. Traditionally skin pigmentation is believed as the most important photoprotective factor, since melanin, besides functioning as a broadband UV absorbent, has antioxidant and radical scavenging properties. However, UVB induced melanin provides coverage against subsequent UV damage via increased melanin production supplemented by the redistribution of melanin towards the upper layers of the skin, whereas UVA-induced tanning which is a result of photooxidation of existing melanin substrate provides very little coverage in the way of photoprotection. Neuropsin is the UVA skin/cornea photoillumination receptor. Although UVB and UVA portions of solar spectra are very well studied, there is a lack of published studies on the effect of visible light of pigment induction in the skin. Considering today’s blue-lit world this is something of a black hole in the literature and is the focus of this webinar.
Melasma is an uneven type of pigmentation of the skin of women. Recent studies have shown that 470 nm light is especially capable of causing melanogenesis even when UV light is subtracted. 470 nm light is in the blue color frequency.
Interestingly multiple exposures with VL has been shown to be able to induce pigmentation in explants extracted from the Caucasian skin. Further exploration of biological endpoints suggested that besides pigment formation due to photo-oxidation activities, VL was able to activate the whole melanogenesis process in skin. This information has not reached the clinical dermatologic/opthmologic practice. Considering how much blue light is present in the environment this recent finding has massive implications. The clinical result of a recent study confirms the ex-vivo studies and demonstrate that VL is able to induce pigmentation after multiple exposures, which suggests that preconditioning is required to activate the melanogenesis process. Technology clear allows for multiple exposures. The findings also align very well with the findings from Mahmud et al., since both studies demonstrate that VL cannot produce persistent pigmentation with just one VL exposure, especially in subjects with Caucasian skin.
Taken together these recent results demonstrate that VL can have a significant impact on producing “uneven pigmentation in skin” (melasma). This pigmentation is the main factor in photoaging. No longer can we blame UV light as the source of photoaging. Furthermore, there is now the first human reports in the literature that preconditioning of the skin with VL sans UV, followed by multiple exposures to VL, can result in uneven pigment formation. Thus photo exposure and photodamage should not be considered strictly as a result of UV exposure since the skin is exposed to whole spectra of wavelengths including VL, and VL can induce photodamage pathways in a manner similar to UV. People should also remember that all modern indoor lighting subtract out UV and IR light further pointing the cause of modern skin pigmentation to overexposure to blue light.
Red light has been shown to lower the risk of melanogenesis but this color light has also been subtracted from modern man-made light further increasing the blue light hazard for skin pigmentation. Even light-emitting diodes at 830 and 850 nm have been shown to inhibit melanin synthesis in vitro. you’d think the skin doctors would get this information to women with melasma but it does not seem to make it to the public.
Although photobiologic studies of sunlight date back to Sir Isaac Newton in 1671, most available studies focus on the UV radiation part of the spectrum. The effects of visible light and infrared radiation have not been, until recently, clearly elucidated. You need to be aware of this “hole” in the literature.
So what else in the literature have been forgotten?
I want to start with historical stories about Dr. Ignaz Semmelweis and Dr. John Snow a British doctor. Semmelweis and Snow used epidemiology of trends to solve major diseases that were afflicting the people of their respective times.
In the early 1800’s infections were the leading cause of death and infections were believed to be caused by something called miasma or bad air, not germs. Microbes were discovered 150 years earlier but the toxic mist of air was thought to be more likely an etiology. This miasma was not thought to be transferred by physical contact. At the time, hospitals were the new human invention to help the public good, but they were the earliest incubators of disease because they were indoors and those who attended them risked their lives for treatments they needed for trauma or thought they needed for chronic conditions. Prior to this time babies were born in homes with midwives.
By 1840, 32% of women giving birth in a hospital died. Doctor’s, all male at the time, blamed their patients for those deaths. Semmelweis looked at the problem differently at Vienna General. It turned out he recognized that women in labor were admitted on alternate days to two different clinics. One was run by doctors and the other was run by midwives. He noted early on that childbed fever seemed an epidemic in the doctor’s clinic and not in the midwives clinic. The women in labor knew it too. They would wait even with children hanging from their vagina until midnight to be taken care of by the midwives. Semmelweis found that 2-8 % of new mother’s died of childbed fever cared for by midwives. It was over 60% in the doctors’ clinic. He looked at both clinics for answers to the paradox. In 1847, a close friend of Semmelweis and a former doctor himself was cut accidentally by a student’s scalpel during an autopsy. He died of childbed fever. Semmelweis knew why doctors were killing their patients and not midwives immediately. Doctors would pass time by going to the morgue and teaching students anatomy on corpses. Midwives never did this. He thought that something in the morgue was being transferred to the maternity ward.
In this time doctors would wash with chlorinated lime to get rid of the stench of death on them. He reasoned what if the washing of the hands with the same material could remove the vector of death for women. He instituted a policy of hand washing for doctors and within one month the incidence of death from childbed fever was equal in both clinics. This made him very unpopular with the doctors of his time because it showed clearly that their behavior was the proximate cause of their deaths. It wasn’t 20 years later that Pasteur innovated the germ theory and it was proven by Robert Koch, where Semmelweis was vindicated.
By this time Semmelweis was long dead. Since he rallied against the establishment he was lured to the insane asylum by another MD about seeing patients who were sick as a setup, and when he arrived, he was forced to drink castor oil and then beaten by guards and died two weeks later of sepsis. His colleagues wanted this new information buried from the public. Germ theory proved him right but it did Semmelweis no good. Being a leader or smarter than others is good in some ways but not in others especially if you are way out in front of the paradigm.
At the same time, miasma was killing women, many bad fluids from hospitals were being dumped into water supplies. In August of 1854 residents of London’s Soho district began to fall ill in large numbers. They developed explosive diarrhea which was watery and white and it never stopped. Each patient would produce 20 liters of stools per day which was dumped in the cesspools below their cramped houses in Soho. They all had cholera.
Snow was skeptical of the “miasma story” circulating in Europe from Semmelweis time and was looking for an alternative explanation. He believed the illness was waterborne. He interviewed Soho residents and mapped cholera outbreak and survivors. Snow realized quickly that the water pump on Broad Street (now Broadwick Street) was the source of the epidemic. He used rational logic and evidence he had at that time, to solve the issue. Mind you he never was able to culture cholera from the water supply because we did not have the ability to do such things in the 1850’s. His work led to the disabling of the water pump and he went on to chlorinate the Broad Street pump. This is how water sanitation took hold in all of Britain late in the 19th century. This is where water fluoridation ideas first got its foothold.
The Industrial Revolution, which took place from the 18th to 19th centuries, was a period during which predominantly agrarian, rural societies in Europe and America became industrial and urban. Prior to the Industrial Revolution, which began in Britain in the late 1700s, manufacturing was often done in people’s homes, using hand tools or basic machines. Industrialization marked a shift to powered, special-purpose machinery, factories and mass production. The iron and textile industries, along with the development of the steam engine, played central roles in the Industrial Revolution, which also saw improved systems of transportation, communication, and banking. While industrialization brought about an increased volume and variety of manufactured goods and an improved standard of living for some, it also resulted in often grim employment and living conditions for the poor and working classes.
For the first time in human history, people went from working outdoors to working indoors.
When I thought about blue light and nnEMF I decided to embark on finding the real cause of neolithic diseases. I did not have to look far to find a huge missing piece of data ignored by the modern paradigm. The industrial revolution lasted from 1760-1840. This began to change mtDNA inheritance because people began burying the sun by living an indoor existence causing a spectral deficiency in light radiations. Here we saw outbreaks of TB in Europe and rickets in the working children. These were all diseases of darkness, both treated very successfully by sunlight.
In 1900, the average life expectancy across the whole globe was 31 years old. Living in a developed country afforded some benefit: they lived to 50 by 1900. Humans for our entire evolutionary history managed to live 20-30 years but the average life expectancy would have been lower. The figures are highly affected by infant survival. In 1900, 3 of ten children died before 5 driving the average life expectancy dramatically lower. In fact, if infant mortality had remained the same in 2000 as it was in 1900, over 500,000 infants would have died per year in the USA per year before their first birthday. Instead, only 28,000 per year died. That benefit is given to vaccine and antibiotic development but my intuition told me it was the child labor laws in the early 20th century that was a larger benefit. It got kids out of factory jobs and back outside and in schools. Today, kids are being locked up in schools for 8-10 hours a day under blue light with Wifi towers in the classrooms and hallways. Many now have Cell Towers installed on the roof to make money. This might be why today’s epidemiologists are finding some interesting links of mitochondrial diseases in school-age children.
One thing was clear from my research, in 1900 infectious disease top the list of killers of humans. Flemming and Florey got us penicillin in large amount by WW II in 1944.
So what did I see in 2000? Our 21st-century lives are now a sterile ceasefire with massive vaccine programs and antibiotic use, water sanitation via chlorination and fluoridation and more hygiene medical practice. What was the human condition? Today infectious disease remains a top ten killer, but not at the very top as it was in 1900. Today, the top killer is neurodegeneration and heart disease closely followed by cancer. Previously rare or unheard of conditions have now risen to prominence from nowhere like diabetes, obesity, and autoimmunity. These neolithic diseases are now considered being a normal part of human life today. This raised the question, what if they are not normal human diseases of aging? What if these are all diseases tied to a loss of energy/information flow from mitochondria heteroplasmy? What drives mitochondrial disease? Environmental change to the maternal germ cell line. We got that answer from Dr. Doug Wallace’s work in the last 40 years. This raised another question in my mind, “what if the environmental change since 1880 has fostered the diseases by epigenetic engineering due to some man introduced to Earth?” I began to channel my inner Semmelweis and Snow.
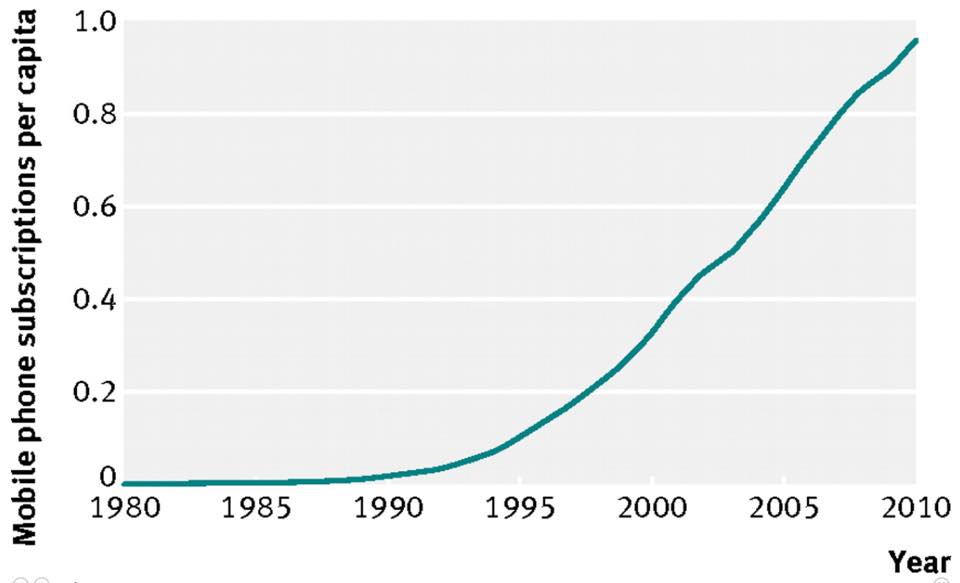
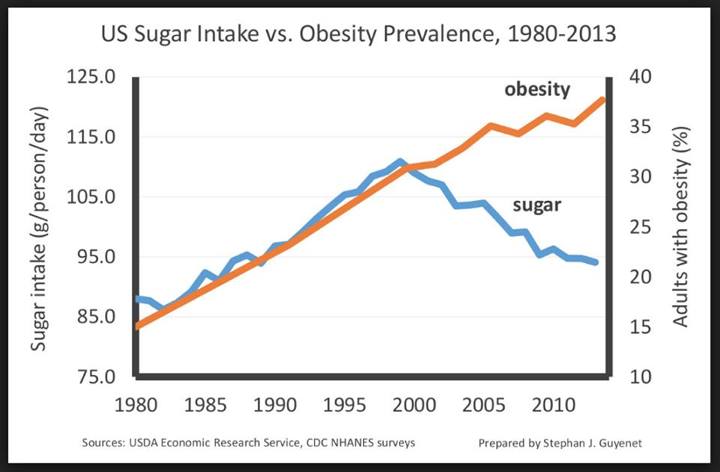
Today your friends and family won’t have smallpox, cholera, or polio. Instead, you’ll see allergies, hayfever, diabetes, autism, hypothyroidism, cancer Alzheimer’s Disease, Parkinson’s Disease, and Multiple Sclerosis exploding. Obesity is a global pandemic now in 50 years. Look at the cell phone graph above now. The spike in artificial light really ramped up when humans began using a cell phone on a massive basis, but the artificial light behavior of humans began around 1880. Many people want to blame sugar as the cause of the obesity epidemic, but take a look at the graph below based on NHANES data. Sugar does not really explain the spike but the one tied to artificial light certainly does fit the modern obesity epidemic. Fake light drive blood glucose higher, so one can get the clinical picture that people appears to have high blood glucose and high insulin levels when in fact they are not eating huge amounts of foods that are sugar related or become sugar in our bodies. This throws a major monkey wrench into the current Low carb high-fat paradigm. We should not be blaming food here. Could it be, that modern lightening and technology are capable of ruining mitochondrial functioning to give us the appearance we are all massive consumers of sugar? That is what the webinar is all about.
Allergies, autoimmunity, neurodegeneration, digestive troubles, mental health, and obesity are the new normal for man. When I looked back at the data I found allergies and asthma were rare in 1930. By 1980, it shot up so quickly that every class had at least one kid with a peanut allergy or asthma. Today, it’s now up to ten percent of the class!!!!
What about an autoimmune disease (AI)? Autoimmune Type 1 diabetes affects 1 in 1000 people and is easier to recognize that type 2 diabetes (T2D). What is extraordinary about type 1 autoimmune diabetes is that it is a NEW disease of modern medicine. Most physicians do not even know this. Mass General has extraordinary records for the US for 75 years in the 19th century up until 1898. I reviewed their logs. In those logs they only record 21 cases of type 1 diabetes in 500,000 cases they saw in 75 years. It was not a case of missed diagnosis either because the symptoms of Type 1 diabetes are easy to see clinically. In fact, not one autoimmune disease were in the top 20 diseases that afflicted humans in 1900. Today AI’s makeup 15 % of global causes of human disease. After WW II formal record keeping improved. In the UK 1-2 children in every 5000 were afflicted in the US, Canada, and the UK. The war did nothing to alter the disease but soon after the war cases began to rise. By 1973 diabetes was six or seven times as common as it was in the thirties in those countries. What changed between 1930-1970’s? We began to use artificial light to see indoors and extend the use of light frequencies to modern communication. This is when RF and microwave use began its massive ascent in the West, specifically in the USA.
MS now affects twice as many in 2000 as it did in 1980. Celiac disease is now 50 times as common as it was in 1950’s. Lupus, Rheumatoid Arthritis, Inflammatory Bowel Disease are all at least doubled in the last 25 years. The obesity epidemic took off in 1950 in the US according to most data I’ve pulled. In the US we started to collect “data on fatness” in 1950. The first survey was done in 1960. 13 % of adults had a BMI north of 30 in 1960. 30% more were at a BMI of 25-30. By 1999 30% had a BMI north of 30. Today 64% are now above 30 on a BMI scale!!!! Trends in the UK are the same as those in the USA. Most food guru’s, doctors, and researchers want to blame certain foods for this obesity trend but this graph show you this might not be wise using NHANES data. What else changed in the human environment on a global scale from 1960 onward? This is when Intel began making chips to power the coming tech boom. It first began with companies employing wealthy middle-class Americans but rapidly spread to all classes by 1990.
What about the new diseases that we never saw in 1900? For example, in the 1940’s autism was so rare it did not have a name. Record keeping began in 2000 with this disease. In 2000 it was half as common as it is today. Autism rates used to be 1 in 500 and today they are 1 in 68 kids, but 1 in 42 boys. In some locale’s, like Orange County, California, it is now 1 in 30 males births.
At the moment it is fashionable to look at genetics for the causes of all diseases but if you understand genetics there is no way that in 5 generations genes will change that much. Not one study shows this rapid change so why are we looking there? We know the nuclear genome cannot change this quickly.
This raises the question, “What genome can change rapidly?” Prokaryotes, viruses, and Archea are known to and observed to do this. People forget mitochondria might have a bacterial origin and they way they work remain more bacterial and less eukaryotic. People forget humans are a species whose cells still contain two genomes. We have a nuclear genome that is related to HERV viral parts and we have a mitochondrial genome that we usurped from a bacteria 600 million years ago. The Human Genome project shocked most of the world because it showed we have a lot fewer genes then we all thought. It also should have been the wake-up call that we should stop looking at genes for modern day diseases. I decided to use Semmelweis and Snow’s ideas to see if mitochondrial damage from the electromagnetic spectrum might the smoking for new neolithic diseases.
Epidemiology is a mainstay of medical detective work. It is simple if you understand what Semmelweis and Snow did. They asked 3 main questions in solving the problems they faced in their time. They were:
1. Where are these diseases occurring?
2 Who do they affect?
3. When did they become a problem?
The answers to those three questions can help answer where we should be looking for the causes of 21st-century diseases. For Snow Where was the biggest clue to the mystery of the Broad St. pump. Today we know allergy, autoimmunity, and obesity all began in the western world. The epicenter of obesity is in the southern USA where I live. Geography does not explain it all. All Neolithic disease began in the West but they have spread globally fast. The clearest particular correlate of the topography of diseases is wealth. It has been often shown that for every 10% increase in tech spending the world gets sicker and fatter. NHANES charts (above) are linked in a linear fashion to tech spending. One thing is clear from 1950 onward, with wealth creation comes chronic illness. In fact, the size of your salary, the wealth of your neighborhood, and the status of your country all contribute to your risk of these diseases. Modern epidemiologists have found many links to zip codes to specific DRG codes in hospital data but no one seems to understand the linkage. I think I do. That is what this webinar is about. It is my Semmelweis/Snow moment working for you, my members.
The other questions Snow and Semmelweis asked were:
Who does these diseases effect?
We learned “Who” was important in the 1918 pandemic of flu. That flu killed young healthy men more and spared the old and children. Why? The immune response was so strong from a competent immune system it caused a cytokine storm that killed the people you least expected to die. “Who” is a question that tells us why something is dangerous.
“Who” is composed of 3 elements:
1. ages of those affected.
2. races affected.
3. sexes affected.
Age of neolithic diseases tells us way more disease is afflicting younger ages. Autism, allergies, IBD, MS, diabetes, and obesity are affecting young and younger population. Disease acuity is shockingly young today. If you do not believe it ask any ER physician.
Races: Blacks Hispanics and South Asians are more fat and have higher cardiovascular diseases than whites in the western world. Allergies and asthma affect more blacks and autism and autoimmunity is a wash with respect to race. Sometimes what appears as a racial difference is buried in migration patterns. The best way to untangle ethnicity and environment is to look at the health of recent migrants in human history to the USA. I have. In the 1990’s civil war lead to a mass exodus of Somali blacks to North America. That diaspora faced a new battle: While autism is rare in Somalia the incidence of the migrant’s children rapidly jumped to match children in North America. This was evident in Toronto when it was studied. In Somali’s immigrants, they have specific cultural names for autism here. They believe autism is a Western disease. The same was seen in Somali’s in Sweden. Race is not the key but location from the equator seems to be. Somali is 5 degrees North of the equator and is a poor country with low tech penetration.
What about sex?
Do women and men suffer equally? Women have a stronger immune system because of childbearing but it appears this superiority causes them to have more autoimmune conditions. Women suffer the bulk of modern AI’s. Allergies affect more boys than girls but after puberty, it switches and girls have more allergies. Gut disorders affect women more than men. IBS is twice as common in women than men. Obesity afflicts women more than men. Mental health afflicts women more than men including depression, anxiety, obsessive-compulsive disorder. Autism is a male predominant disease.
When you look at it with 21st-century eyes, there is a clear female bias in modern plagues. These diseases are not diseases of old age. They are not diseases of genetic inheritance. They occur as diseases of the privileged young with good immune systems, and they tend to be female.
The last question to ask: When?
When we look at the best record keeping in Scandinavia it appears 1950-59 is when disease phenotype began to explode. Most experts look at the end of the WW II as the inflection point. In my opinion, either one fit the etiology of the source. From asking What?, Where?, Who?, and When? we have established several key things for 21st-century diseases.
The disease often arises in the gut, are associated with immune systems. Second, they strike the young, often children, teens, and young adults and many more women than men. Third, these illnesses occur in the Western world but now are quickly spreading to even rural cultures at fast speeds as they modernize. Fourth, they began their rise in the West in the late 1940’s and developing countries followed suit in a linear fashion.
The key is the gut link and speed of transmission to these diseases. It mimics how a bacteria reproduce. Bacteria grow fastest under nnEMF as NASA space programs have shown modern space medicine. This was originally discovered aboard the MIR spacecraft by American astronaut David Wolf in 1998. The female link ties this to mitochondrial biology because all mtDNA is maternally inherited and this makes sense why children are inheriting high heteroplastic mtDNA from mothers in bad environments.
I will remind you again, we have two genomes in us, one bacterial that controls energy flux in tissues and the other virally based that controls nuclear-based genes. The bacterial one mutates 5 times faster than the other and it shows maternal inheritance. It is massively affected by nnEMF and light environments with spectral deficits compared to sunlight. Many scientists will want to blame the microbiome changes as the cause of the diseases but they often fail to recognize how mitochondria have their own network of bacterial genomes working inside of our cells to work or fail to release massive amounts of light for signaling compared to eukaryotic cells!!!!!
We are 10% human, 60% water, 10% magnetic, and 20% solar lit. Mitochondria and bacteria respond differently to these set of “environmental affairs” tied to light, and I believe it explains why 21 st century disease really exist. This is where Semmelweis and Snow’s sleuthing has led me.
So what happens when we block parts of the spectrum of the sun or get too much of parts we are not supposed to experience? Can light cause digital toxicity?
Do you know when this “light assault” really began on human mitochondria? Way longer than most of you would guess.
Humans have always wanted to look attractive. Even in ancient times, people desired to avoid sunburn. This takes us back to the Egyptian days. Egyptians always considered light skin more beautiful than dark skin. However, Egypt’s sun-drenched environment made it difficult to maintain light and radiant skin. Recently, the papyri and tomb walls were translated and this revealed that the Egyptians used the ingredients of potions to ward off tan and also heal damaged skin. This is why the Egyptian mummies have been found to have the same diseases we see today. The slaves of this empire were far healthier than their masters. The irony was that “Ra” was their God and their vanity blocked them from “his wisdom”.
The Egyptians used ingredients that have been rediscovered by modern scientists. For example, the Egyptians used rice bran extracts in some of their sunscreen formulas. Today, gamma oryzanol is extracted from rice bran and is used as in industry for its UV-absorbing properties. The Egyptians also used jasmine in their version of sunscreens. Recently a study revealed that jasmine helps to heal DNA at the cellular level in the skin and also mends skin damage. A lupine extract was also used by the Egyptians to lighten the skin and all these ingredients are still used in our sunscreens.
In the early 1930’s, a South Australian chemist, HA Milton Blake, experimented and produced a sunburn cream. Following this invention, the founder of L’Oreal Company, chemist Eugene Schueller refined the invention and the first sunscreen made its debut in 1936. Guys, 1936 is only 80 years ago. This is right before the modern spike of all the neolithic disease we see by NHANES data.
Later in 1938, a famous chemist called Franz Greiter developed a cream which he named as Gletscher Crème or Glacier Cream. He also came up with something called as the sun protection factor which is now known as SPF factor in a sunscreen. Franz invented the SPF factor which then became a standard for measuring the effectiveness of sunscreen when applied at an even rate of 2 milligrams per square centimeter. The initial Glacier cream contained SPF of two. This formula was picked by a company called as Piz Buin.
Post this, many others tried experimenting with the sunscreens and many variants made their debut. In 1944, Florida based pharmacist, Benjamin Green patented another version of sunscreen. He called it as Red Vet Pet, and his patent was bought by a company called as Coppertone who sold it as “Coppertone Girl” and “Bain de Soleil” in the early 1950s.
Finally, in 1980, Coppertone developed the first UVA/UVB sunscreen which has been in the markets with different names.
Scientists are still searching for more effective ways to protect the human body against the sun. In my opinion, they should stop. The best way to protect yourself from the sun is to look deep into the wisdom that built the Epi-paleo Rx. One goal of these scientists is to develop a sunscreen pill. My goal was to find out how primates in the equatorial sun did it to lose their hair in the East African Rift. Shellfish was that answer. Recently, significant attention is been given to a substance called astaxanthin that is found in red ocean plants and marine animals, such as salmon and crabs. Astaxanthin is considered as the most effective protection against free radicals found to date in nature. Astaxanthin is an antioxidant that helps in reducing the pain and swelling associated with sunburn too. Did you know that? Most humans do not. Sometimes humans capture lightning in a bottle.
For the eye, the change is not back to the Egyptians. It is a relatively recent change when we look back. We have data that in prehistoric time Inuit peoples wore flattened walrus ivory glasses to block harmful reflected rays of the sun, the earliest historical reference to sunglasses dates back to ancient China and Rome. The Roman emperor Nero watched gladiator fights through polished gem lenses.
In China, sunglasses were used in the 12th century or possibly earlier. These sunglasses were made out of lenses that were flat panes of smoky quartz. Quartz allows UV light penetration. They offered no corrective powers nor they protect from harmful UV rays but did protect the eyes from glare. Ancient documents describe the use of such crystal sunglasses by judges in ancient Chinese courts to hide their facial expression when they interrogated witnesses.
James Ayscough began experimenting with tinted lenses in spectacles around 1752. This was when eyeglasses became fashionable for humans. Ayscough was steadfast in the belief that blue-or green-tinted glass could potentially correct specific vision impairments. Protection from the sun’s rays was not a concern at this time.
Glasses tinted with yellow-amber and brown were also a commonly-prescribed item for people with syphilis in the 19th and early 20th century because one of the symptoms of the disease was sensitivity to light.
In the early 20th century, the use of sunglasses become more widespread, especially among the early Hollywood movie stars of nontalking black and white pictures.
Inexpensive mass-production of sunglasses started in 1929 when Sam Foster introduced them to America. Foster sold his sunglasses on the beaches of Atlantic City, New Jersey under the name Foster Grant from a Woolworth on the Boardwalk. These sunglasses were made to protect people’s eyes from the sun’s rays. Foster-Grant sunglasses became the first cultural trend to wearing tinted lenses that altered the solar frequencies.
Polarized sunglasses first became available in 1936, when Edwin H. Land began using his patented Polaroid filter when making sunglasses. This was adapted from cameras. Since the eye was viewed as only a camera no one understood the potential biologic effects.
Sunglasses even played a significant role during the World War II, when Ray Ban created anti-glare aviator style sunglasses, using polarization. Ray-Ban Aviator sunglasses became very popular with the celebrities and the community in 1937 when they started to be sold for public consumption.
THE ELECTRIC POWER WARS AND LIGHT BULBS GAVE US A SPECTRAL DEFICIENT ENVIRONMENT
Society became artificially lit by Edison and Westinghouse bulbs in the late 19th century (the 1880’s) and the effect was extended by Tesla’s AC induction motors for cities in 1893. This made nighttime light a luxury item everyone wanted for the first time in human history. This is only 123 years ago. Cancer in 1893 was almost unheard of in medicine. That seems important since the sun power has remained constant since the Cambrian explosion.
Today, sunglasses with UV protection has almost become an industry standard, and there are a lot of tints available for sunglasses, and sunglasses styles are changing every year. The same is now true for eyeglasses and IOL implants.
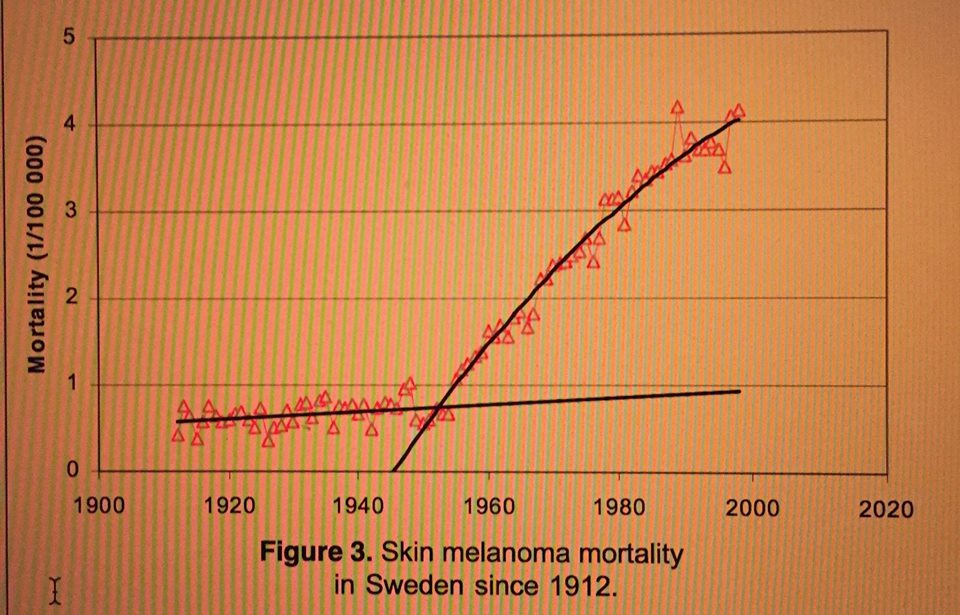
What about skin cancer? For this link to light, we must turn to the best record keepers on the planet: Sweden. For those of you who don’t know Sweden as a country keep meticulous records of the population and has for close to 120 years. So when we want to use epidemiology to spot trends this is where we should head for reliable data.
MELANOMA IN SWEDEN
Figure 3 shows the mortality for skin melanoma in Sweden. Data before 1955 is not published by the authorities but was retrieved from a library. The raw data shows that the natural death rate increased from about 30 per year in 1912 to 50 in 1954. Consider what I said earlier about the use of eyeglasses and sunglasses and sunscreen (1936) at this time and understand that Hollywood was the only game in town before TV was invented for human entertainment. Do you think people got the idea to wear sunglasses from famous humans they wished to emulate? Are humans not social parasites with behavioral trends? Isn’t this why we have Madison Ave. and Bulletproof executives nowadays? This gives an increase of 0.5 more victims per year. From 1955 it increased to 325 in 1996, which gives an increase of almost 7 victims per year, i.e. 14 times more than before 1955.
Take a look at this hyperlink. In Sweden where the quantum yield is low epidemiologic conclusions showed the age-specific incidence of malignant melanoma of the skin appears to be following a pattern of response to an imposed environmental change that occurred in 1955. Researchers believe that the frequency modulation (FM) broadcasting radiation at whole-body resonant frequencies is likely such an environmental stress. FM is part of the electromagnetic spectrum.
Several cancers correlated with skin melanoma in the 26 different Swedish counties, but leukemia was not one of them. I found this interesting because of how the sun affects the skin and blood simultaneously because of the nitric oxide effect. A closer look at the lung cancer mortality from the hyperlink above shows a development very similar to skin melanoma (see Figures 3-4). The average consumption of cigarettes in Sweden decreased from 1,946 cigarettes per year per capita in 1980 to 1,200 in 1995, although the mortality has continued to increase; however, the increase has been lower than that for skin melanoma. In Figure 19 they plotted the annual melanoma deaths vs. lung deaths in Sweden for each year from 1912 to 1996 (beta = 0.982). In order to test by other means if lung cancer and breast cancer are related to skin melanoma, the researchers combined two databases: the Swedish Cancer Register and the Death Cause Register of Sweden. The records of those who died from breast cancer or lung cancer were searched for any treatment for skin melanoma earlier in their lives. As a reference, all other death causes except breast, lung or melanoma cancers were also searched for the same. A specific, non-cancer death cause was ischemic heart disease, which also was searched for any melanoma treatment. The data was collected over the time period 1970-1998. The results show the fraction (%) of the deceased who earlier in life had been treated for skin melanoma: All death causes: … 0.21% (>2.5 millions deaths) Breast cancer: ……. 0.37% (42,610 deaths) Lung cancer: ………. 0.33% (71,956 deaths) Heart Disease: …… 0.24% (821,367 deaths)
The researchers concluded that breast cancer and lung cancer are somehow linked to skin melanoma (by light frequencies), since people who died due to breast or lung cancer had an increased melanoma incidence by a factor of 1.67 (0.35/0.21).
This was further underscored by the strong geographical relationship between melanoma incidence and lung, breast or colon cancer incidence. The large numbers involved in this analysis exclude the possibility that the results are just a matter of coincidence. Figures 20 and 21 show that colon cancer relates to skin melanoma and that lung cancer and bladder cancer are strongly correlated “by some environmental source.” Figures 22 and 23 show that cigarette consumption is not a strong common factor for these cancers. See Table 2, data is from 1989-1993 in the above hyperlink.
What about the situation in the US? Data is not readily available and I think it is by design. Look at this hyperlink from the EPA about Washington state: The US map shows that the further from the equator one is the more melanoma shows up. Does this make sense based on what dermatologists/opthmologists are telling you presently?
These places are where UV indexes are very low. In fact, no place below Jackson, MS makes UV light between May 15- Sept 15 24/7 in the USA. This raises the question why is melanoma so common in a place like Washington? Have we missed something critical? Do you remember that Washington has a large technology company based there (Microsoft)? The map appears to tell us that those out of the sun inside may have the highest risk of cancer because they have no UV light and a ton of indoor light exposure. Where I live skin cancer is not common and neither is melanoma. So what do you believe? In the link I just posted new cases of melanoma in the state of Washington showed the rate of new melanoma diagnoses—responsible for 75% of all skin cancer deaths—was 35% higher in Washington than the national average from 2001-2005 and was the 5th highest in the U.S. Does this make sense based upon what skin and eye doctors are telling you about sunlight?
I decided to dig deeper like Semmelweis and Snow did face with this data for you.
We are perfectly adapted to the radiation of our sun on Earth by evolution. This becomes obvious when you look at the medical studies on light use prior to the advent of antibiotics. The data of this time clearly show the advantages and achievements of heliotherapy and heliotherapy specifically refers to solar radiation therapy that living things get naturally. Today, living things no longer get those radiations and this is where diseases like skin cancer have exploded. Heliotherapy is sensitive and specific to cells in their dark mode because we should be using sunlight directly without altering its frequency footprint, without removing parts of the spectrum as modern man has done. Corporations (GE and Phillips) removed UV and IR light to save energy and money, but never thought to test how this version of light would affect living things by subtracting frequencies. This ability has created the situation that has allowed medicine to formalize the beliefs in a dogma that solar radiation causes skin cancer and eye diseases when in truth these diseases showed up once Edison, Westinghouse, and Tesla began creating artificial light to allow man to live inside and at night beginning in the 1880’s. Modern communication began using other light frequencies to communicate after the success of radar in WW II. This was in the 1950’s just when the obesity epidemic really powered up. It also is when heart disease started killing Americans and why people like Ancel Keys started to blame fats for the cause. Prior to this time, the incidence of skin cancer, melanoma, and diabetes was rare. Darwin was correct about his principle that survival of the fittest means that we humans, at the moment – are the fittest on the planet when we are absorbing a chronic non-linear stimulus of sunlight for our physiologic function. In fact, this means we are adapted to sunlight as a complex non-linear stimulus via cells, EZ water and via our mitochondria. What does it means when the light you live under is man made?
This adaptation process means if you take away the non-linear stimulus for any reason, rightly or wrongly, the effect will be magnified in our phenotype and/or disease presentations. This marries beautifully to what Dr. Doug Wallace has shown us in mitochondrial medicine for 40 years. In the past, we have many instances where burying the sun was responsible for a good number of specific body reactions. We saw this in tuberculosis and rickets in the later 19th century when Edison and Westinghouse were making light via light bulbs and illuminating darkness for the first time in a sustained fashion in man’s history. It was then that epidemiology of disease showed that humans began having problems.
At this moment in time, most human neolithic disease showed up in non-linear fashion too. They were not common 1880-1940 because this was when maternal heteroplasmy rates were initially beginning to affect their germ cells lines which would eventually become their future offspring. This means that their children would be born with higher heteroplasmy rates than any other human generation before it. This mitochondrial genomic action has sped up from 1940- 2016 because of how mtDNA controls heteroplasmy rates on the maternal side. This explains why women and children are now afflicted with the disease much more so than any other group today. It should be clear does anyone with an understanding of mitochondrial and prokaryote biology that human systems need the non-linear physiologic solar stimulus at a certain dosage to keep our system running properly. Today, we are blind to this because we truly do not understand that most of the sunlight’s effects are non-linear on dark mode plasma in cells. Vaccines mimic the physiologic effects of the sun. In fact, I now consider the sun as nature’s best vaccine. Modern medicine credits vaccines/antibiotics for the expansion of life expectancy in the 20th century, but could it be that we need them today because we have lost the non-linear effects of the sun from our lives?
Consider TB and rickets in 1890: When you look at the pictures of the sick children from that moment in time, and after one year, they were completely healed before the advent of drugs or vaccines (it’s just proved by their picture because this is what we have to judge what happened these days), you can see that in a healthy body, there for sure is a healthy immune system as well. Quinones are chemicals that have been collected from meteors that fell to Earth from interstellar space. Quinones have structures nearly identical to those that help chlorophyll molecules transform light energy into chemical energy in leaves plants. Mitochondria use quinones in its Q-cycle (Dec 2016 webinar) to tunnel electrons to the ATPase and to reduce oxygen. Sunlight exposure, it’s definitely much, much more than tanning. Tanning is just what you see, what is visible on your skin. What happens in your mitochondria and in your blood plasma is far more illuminating to the curious mind. The color tone of your skin comes from the melanin response in your skin and this links to your mtDNA haplotype and the solar exposure of your epigenetic history. It’s also the reflection of the light being emitted from the cells of your bloodstream. Since humans migrate outside of the borders of their mtDNA haplotype the circadian mismatch that is possible are endless. This has created the perfect storm for modern disease generation. If your skin is exposed to sunlight, you will experience some invisible changes in your circulatory system. The capillaries, for example, they will be modified under the influence of sunlight. The skin is closely linked to the autonomic nervous system (ANS). It’s a kind of an external organ of the vegetative system in your body.
For example, when you live under chronic summer conditions at the equator, we need much more water in our system in order to produce enough sweat, in order to cool down our body. We also see a different tone of skin and a radically different mtDNA haplotype. This means that sunlight not only influences the skin, but it influences all the inner organs as well. It’s a kind of a quantum concert that affects all things with a deep prokaryotic history in living things. All of these are started by the stimulus of the sun or the absence of the stimulus from sunlight. This makes sulfated vitamin D3 is a kind of seasonal stress hormone for those who live outside the equatorial zone. Inside the zone, it is chronically present always and this would select for certain mitochondrial haplotypes. We have other circadian stress hormones related to the production or lack of production of sulfated Vitamin D3. These hormones in our system, for example, are all derived from POMC like the adrenocorticotropic hormone (ACTH, alpha MSH) adrenaline-cortisol blend of certain hormones, which enable us to get up in the morning, to regulate the blood sugar concentration, to be active, and so on. These are the circadian stress hormones. When you think about the different tasks between summer and winter, that’s like reprogramming your heating system in the house, because in summer, the main topic is cooling down the system. You have an intake of 1.5 kilowatts on the square meter, which means if you stay naked out in the sun, your body has to digest a lot of energy, which in the end, is transformed into thermal energy. Cooling is the main task during the summertime and heating is the main task during winter time. This is linked to, for example, the circulatory system. It’s linked to our digestive system and so on.
THE OFFENDER OF MODERN MAN: TECHNOLOGY USES MANY NON NATIVE LIGHT SOURCES TO OPERATE
I view technology as a toxic poison, so the question to ask is, “How long do you want to stay in the poison directly and what potency does the poison have?” There are also many types of poison. Next, look at modern behaviors. They embrace the poison 16 hours of the 24 hours in the day, or maybe even longer if their sleeping space is also compromised. The tendrils of technology have been growing into nature and natural spaces with faux cell phone towers, more powerlines, etc. Even tech-free zones may be problematic with back-reflection into them from population densities. There is something called the minimally effective dose that MD’s learn about in medical school, with respect to toxins. It refers to drugs but is more applicable to sunlight. Talking about sulfated vitamin D3 in a way is a kind of self-given restriction regarding the different processes, which are going on. This is a typical approach we can find in photobiology in the 20th century, which means you are looking for the kind of action in the sun’s spectrum to offset the risk of blue light and nnEMF. The bluer and nnEMF you allow the more solar radiations you need to offset the mitochondrial damage due to the “stretching out of our respiratory proteins”. In the end, when you have a myopic view of light, you find out only ultraviolet B radiation is able to photosynthesize sulfated vitamin D3 in your skin. This means UVB light is a seasonal stress hormone. It really makes no sense blaming this one frequency band of light for skin or eye cancers. If you consider indoor living is more common the further you go from the equator you begin to see humans with nonequatorial mtDNA using fake light and nnEMF to much greater degrees. This is why they become iller than those in equatorial zones. They live a more deficient life from a spectral standpoint. Being indoors at the equator is miserable. As a consequence, when you think vitamin D is the only benefit you can get from sunlight, you automatically will focus on the ultraviolet B radiation. This is why Terry Wahl’s focus on food, and not light is myopic with regards to Multiple Sclerosis.
People tend to focus on what they and their audience can understand. I refuse to do this because if you do you’ll never solve our modern problems. A myopic view does not imply Terry is correct. Your level of understanding has no effect on nature’s non linear laws for light. Look at where she lives and does, with respect to solar light and her indoor life tied to her job and web business. She has no idea about light’s non linear effects in totality when cells are in their dark mode plasma state (August 2016 webinar)
Go have a read of the textbooks and manuscripts of Dr. Auguste Rollier, Albert Schweitzer, Weston A Price, and Finsen as examples for what we are missing today, with respect to light. They all emphasized quite often in their writings that they found that the composition of the different parts of the spectrum are of crucial importance in order to achieve all the benefits you can get from the sun and you can get from staying outdoors. For example, when you look at the cellular effects of ultraviolet B and ultraviolet A, it really depends on the dose if the radiation is beneficial to your system, your skin type, your mtDNA haplotype, your hydration status, If these things are awry for any reason, the radiation can affect biochemistry and may unfold in an odd way causing reactions and/or effects we don’t expect or want. What we can say is that ultraviolet radiation photosynthesizes vitamin D on one hand, but on the other hand, it’s able to damage, and seriously damage cells if the skin tone, solar callus, or mtDNA haplotype are not adapted to the environment they sense presently. It also means these systems can adapted well to altered environments if we understand how they work.
Ultraviolet B can alter the DNA structure directly and indirectly. In the skin as keratinocytes head to the surface, the DNA naturally breaks down and protects us using the Auger effect. What happens if this effect cannot be used because you have psoriasis? You get more skin cancer. Did the sun cause it or did the blue light causing psoriasis cause it? The modern paradigm blames the sun………I don’t because I understand the non-linear effects of blue light to increase skin mitoses. Ultraviolet A can produce and photosynthesize the proper reactive oxygen species in the tissue to marry to mtDNA ROS and RNS. What happens if they don’t because you never get solar light and just man-made light? In order to cope with these side effects, so to say, our skin needs other parts of the spectrum we don’t give it. For example, the near-infrared and the red light, which we find in sunlight in a pretty large amount, these longer wavelengths, they provide metabolic power to the cells. Ultraviolet light primarily is a kind of stress stimulus that harden are a system to harsher light environments. Harshness pertains to UV and IR parts and not the blue parts of the spectrum.
Blue parts never exceed the UV or IR spectrum in sun and we fail to realize these spectral effects on cells. Vitamin D3 acts upon our cells and tissues, and our body makes the best out of it. Our body cannot do that with blue light because this part of the spectrum never exists by itself naturally. If we cannot get rid of the ultraviolet light via our skin tone, our mtDNA haplotype, our melanin level, our body thinks this quantum way, because light teaches cells what to do in these cases they should encounter. When you change the light spectrum to blue, I’m convinced, modern neolithic disease is that result of this change because of its effect on mitochondria.
These diseases become our new normal and we have to make the best out of it or change the light we allow. The normal response would be to make more vitamin D3 for protection but with blue light only and no red we cannot. Sulfated vitamin D3 is a kind of biochemical signaling molecule, which enables a lot of reactions in our body to occur that allows our cells to get by bad times and to cope with the typical tasks that go along with summer, with daylight, or with sunlight. We have no defenses to chronic blue light and when UV and IR are subtracted. When we have on one hand a kind of stress reaction, we can easily imagine that our cells as well need energy in order to answer this stress stimulus
The lack of the ability to make D3 is a sign of a blue light toxic environment. When will MS, IBD, SIBO, cancer, melanoma folks get the message?
EYE MELANOMA ALSO LINKS TO MITOCHONDRIAL HETEROPLASMY?
Uveal melanoma (UM) is the most common malignancy of the adult eye. It is the fasted growing type of melanoma in the world today. It was unheard of in 1900-1950 but its incidence and prevalence have been brisk since the advent of man-made light and sunglasses. The same trend is true in melanoma of the skin. It is far more prominent since 1960 with the advent of sunscreens. Although ocular melanoma is a relatively infrequent tumor, the clinical prognosis is often poor owing to a high incidence of aggressive metastatic disease, for which there are limited treatment options today.
Unlike cutaneous melanoma, however, ultraviolet radiation does not figure prominently among the risk factors for ocular melanoma, but blue light does. UM has a significantly higher incidence in Caucasians than in African and Asian populations. Caucasians have significantly fewer melanocytes than African or Asian populations and their skin type evolved in geographies outside the tropics with solar power was lower. UM arises in melanocytes located within the three different regions of the uveal tract: the iris, ciliary body, and choroid. UM has a median age of onset of 55–60 years. So clearly it takes a lot of exposure to blue light to cause this disease.
EYE COLOR
A correlation between UM incidence and latitude in European populations suggests that lack of ocular pigmentation could be a risk factor for UM, and light iris color has also been linked to poor prognosis in patients with UM. Within populations with light irises, however, elevated levels of choroidal pigmentation have been linked to an increased incidence of UM. So this raises the point how do we stimulate melanin production in cells? Chronic blue light unopposed by UV and IR-A light is the short answer. This is what causes the blue light hazard in the eye. It is also what causes excessive melanogenesis in the skin.
BLUE LIGHT HAZARD EYE:
Systematic literature searches conducted by Ovid (Embase and PubMed) showed that the earliest reports of an association between exposure to blue light and the development of UM have come from in vitro and animal work. Several studies have shown that blue light has a mitotic effect on human UM cell lines. Sunlight exposure does not show a strong association with UM, although arc welding (a source of ultraviolet/blue light) does.
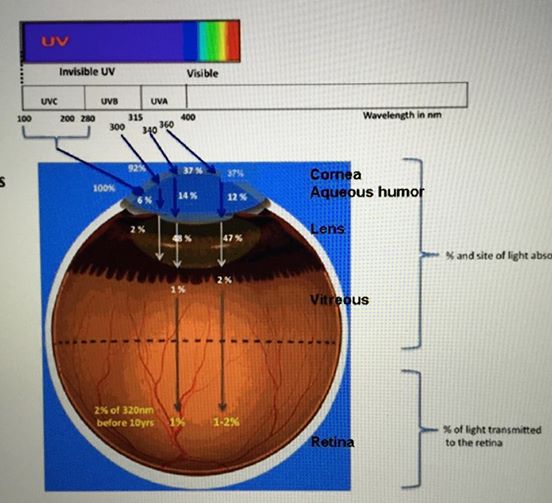
The combined epidemiological/genetic case against a significant role for ultraviolet radiation in the etiology of this disease is consistent with the established properties of the adult crystalline lens and cornea, which is believed to collectively filter out all wavelengths below 400 nm. This picture above challenges that belief now and so do some new data. The recent finding of the UVA illumination receptor in the cornea (neuropsin) however strongly questions this core ophthalmologic belief. Perhaps the key to understanding the link between UM and activities that generate high amounts of electromagnetic radiation (e.g., arc welding and technology use) does not lie in what is filtered out but in what can pass through the lens and cornea. For instance, arc welding produces significant amounts of intense short-wave light in the blue range. Unlike ultraviolet radiation, short-wave (s perceived as blue by the retina) light (400–500 nm) can reach the posterior uveal tract while retaining sufficient energy to be deleterious to biological structures.
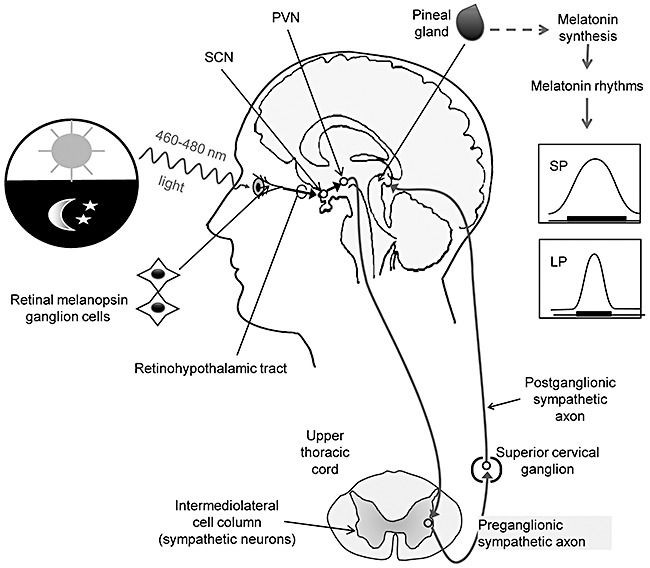
Cultured human UM cells exposed to blue light (peak 475 nm) significantly increased their mitotic division rate relative to blue-light-shielded controls, an effect that was blocked using a blue-light-filtering lens. Although the exact mechanism underlying the relationship between blue light and increased proliferation of uveal melanoma cells remains unknown in the published eye literature, it has been shown in the chronobiologic literature that shorter wavelengths of light can induce retinal pigment epithelial cell death by mitochondrial-derived ROS production. This has serious deletions effects on the central retinal pathways that control growth and metabolism pathways and they also control the production of dopamine and melatonin in the eye.
This interesting observation of blue light to ocular melanocytes was followed up by a study that sought to mimic the effect of blue light on UM cells within the context of the mammalian eye. Human UM cells were xenografted into the eye of an albino rabbit model of ocular melanoma and subsequently exposed to blue light showed enhanced proliferation upon removal and recapture, compared with control samples protected from blue light. The significance of this finding is that the UM cells were exposed to blue light while residing within the choroid, effectively demonstrating that blue light affects uveal cells and can enhance their mitotic ability. This is a crucial step in linking blue light to malignant changes within uveal melanocytes in vivo. The final confirmation of the link between blue light and UM in vivo came from a study in Long Evans rats, a strain with pigmented eyes in which there have been no reported cases of intraocular melanoma. This study described the development of an ocular tumor in one animal following blue light exposure (434–475 nm). This is the range of the melanopsin receptor in the eye known to control melatonin production in the eye to control the entire central retinal pathways (retinohypothalamic tract) to the SCN.
MODERN REFRACTIVE SURGERY
It is believed today, because of the published literature that around 80–90% of blue light at 450 nm can pass through the young lens in children and young adults. Blue light exposure ages the lens much quicker. Today’s modern environment is inundated with blue light because of technology display screens and the change over to LED screens in TV in 2009. As the crystalline lens ages at any age, it yellows and progressively filters more blue light until, by the sixth or seventh decade, blue light transmission can be as low as 20% of that transmitted by the young lens. This aging mechanism is also how the brain protects the retina from aging. Many early onset cataracts are linked to this mechanism. Early types of intra-ocular lenses (IOLs) used to replace the crystalline lens during cataract surgery effectively filter UV but do not block blue light. It is hypothesized that blue light reaching the retina increases the risk of preexisting dysplastic nevi which are the precondition for UM development.
The recent trends in IOL’s are to block 50% of blue light. Blue-light-filtering IOL’s are designed to filter up to 50% of blue light. This models the natural filtering ability of the middle-aged eye, reducing potentially damaging radiation while not impacting on vision. The ophthalmology literature does not seem to realize that blue light bends the more than any part of the visible spectrum that runs human vision, therefore it has little to do with the eye camera vision. Blue light from the AM sunlight, however, is a strong stimulus to pituitary function and hormone release when it is balanced by red light in the sun.
If this concept was better understood by IOLs manufacturers and ophthalmologist, studies would be undertaking to challenge the idea of putting lenses in that block UV light and just 50% of blue. The reason for this misunderstanding is two-fold. Neuropsin presence on the cornea foretells that nature needs UVA illumination exposure from daytime light for maintenance of eye globe health and growth. We know that a lack of sun exposure outside causes myopia to spike and this is associated with elongation of the globe and nearsightedness. This is an epidemic in Asia and Japan where young people are using LED lit screens at an unprecedented pace over the last 25 years. These same adults are now undergoing something called the celibacy syndrome, where they do not want to have sex because their sex steroid hormone release is overdone by chronic blue light exposure via the eye.
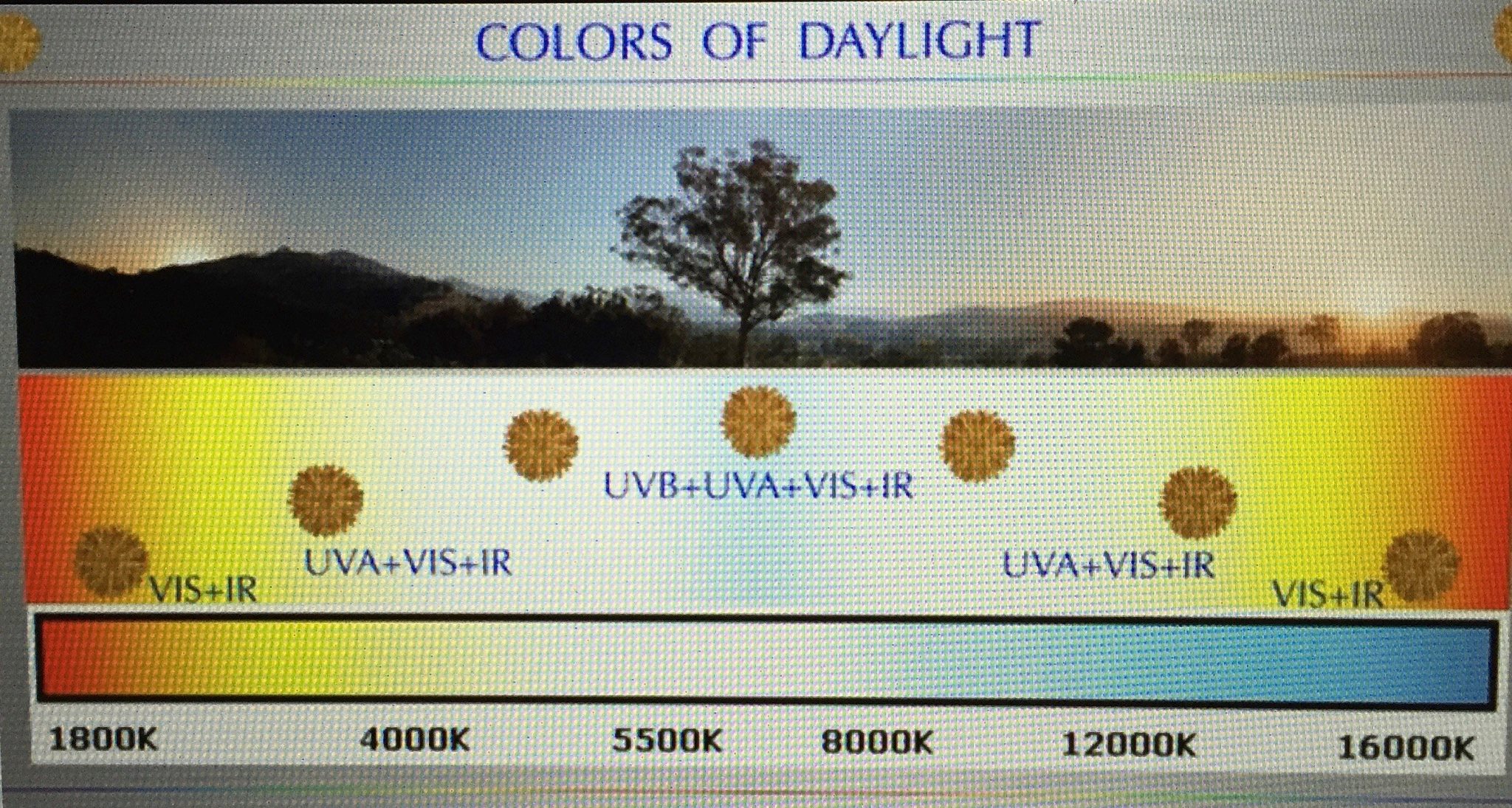
Just blocking 50% of blue may not nearly be enough because sunlight has a tight control on the number of blue light frequencies it contains. For example, at my latitude (28th) 13% of sunlight is blue at Dec 21st and it rises to 26% at the summer solstice on June 21st. The color temperature of blue light is a very powerful stimulus and this helps explain why they eye must have IR and NIR present anytime blue light is present to offset the mitochondrial damage it can cause. Today’s artificial light is created without any stimulus of UVA or IR or NIR as is present in the sun. This abnormal blue spectrum is stimulatory to melanocytes in the eye and skin and correlated with the epidemiological trends in the UM and melanoma. When one considers that neuropsin is also present in the skin of man, this mechanism maybe be behind why skin cancer and melanoma is also exploding since 1960 and was not as prevalent prior to the advent of sunscreens and sunglasses.
MODERN LITERATURE ERRORS
How we study things affects our beliefs and perceptions about things like light. Many researchers have been fooled by the modern animal models used for UM. They believe paradoxically, that 450 nm blue light appears to be phytotoxic to mouse cutaneous melanoma cells. What they fail to realize is that mice are nocturnal mammals and therefore they have scotopic retinas. This means that their photo-attunement and connection to the central retinal pathways will not be tied to the same frequencies as the human retina that is diurnally based. You would have thought this would be obvious when the human photoreceptor that stimulates melatonin production in the eye/skin, melanopsin was found to react to 435-465nm light as the light goes from intense illumination to dim illumination. It has not. Using nocturnal animals to study UM, macular degeneration and cataracts make sense only if you are trying to sell UV blocking and blue blocking IOL’s to clinicians who do not understand the blue light hazard or how the sun connects to the SCN and pituitary gland.
Sunlight makes our surfaces act on a relative basis, physiologically to function by the light frequencies that are present by the hour, day, month and season. Light alters biochemical function below our surfaces because of how it penetrates different tissues. Light penetration by frequency is not uniform and was not designed to be because solar radiation is not constant. And that “relativity” changes the space/time relationships of our cells and tissues and is the basis of circadian control mechanisms in cells. For example, daylight is able to shifts blood into the skin and RPE by dermal/ocular pooling due to eNOS and NO release. The eNOS can affect sulfation and nitrosylation of chemicals in these surfaces because of the frequencies they contain. More than 50% of your blood volume can change your skin surface when the sun is present. In the eye sunlight increase, water flows FASTER between the photoreceptor and circulatory system to the RPE. This is how the 42% of red light in sunlight bridges the large gaps in the macula between the RPE and photoreceptors where our eye camera function is sharpest. The dermal pooling in the eye and skin (UVA) acts to lower our blood pressure. It changes the anatomical structure of the skin by changing the optics of surfaces in the eye. It becomes a sensory stimulus for the interoceptive system to induce biochemical substrates via photosynthesis in plants and changes in the ATPase using red light and water in animals. Sunlight increases sulfated Vitamin D3, histamine, and sulfhydryl groups while lowering (photolysis) adrenaline, steroids, testosterone, estrogen, thyroid hormone, DNA, and RNA. Sunlight induces biochemical reactions via photolysis and it induces coordinated endocrine adaptation effects in the eye and the skin surfaces. It affects the sympathetic and parasympathetic systems simultaneously to tighten the circadian coupling of all growth and metabolic cycles. It is the stimulus for the circadian timing mechanism of the body clock via the central retinal pathways.
It should be clear from the cites below and much of the published literature in chronobiology on the central retinal pathways that all IOLs need to mimic the native crystalline lens. Few understand how Rev-erb links to the blue light UR/IR-A light braking mechanism. It should allow UV penetration because of the newly discovered neuropsin photopigment in humans in the cornea and the amount of blue-blocking needs to be more finely tuned to match the environment the person is now living in. Ideally, the modern world seems to call for IOL’s that are transition lens because of the high risks associated with blue light toxicity in the eye.
There is another consideration that both the dermatology and ophthalmology literature have completely ignored in the construction of their experiments (poor methodology) and why they miss that light is the drug killing us today. New biophysics data have shown that RNA and DNA has an unusual spectral pattern. The current belief in both specialties is that UVA and UVB light is something to avoid. But if we are to accept this belief, why do the skin and cornea have a UVA light receptor in it from birth? Moreover, if UV light is so horrible for human cells to ask yourself why DNA has been shown in thousands of experiments to have a spectrum of fluorescence peak at 350 nm? That peak is 100% in the UV range, FYI. There are two proteins that are tightly associated with DNA/RNA, histones, and chromatin, both have been found by experiment to delay this UV light release in the DNA of melanocytes that lower mitosis in these normal cell lines? This raises the point that UV light exposure may be the breaking mechanism for unopposed blue light via the eye that links it to ocular melanoma.
It also means that lens manufacturers may have left some fundamental bio-physical aspects of light out of their research protocols that is extremely important in the etiology of these eye conditions.
MELASMA and NEONATAL LINKS OF MELANOCYTE MITOSIS:
In infants born with jaundice medicine used to use full spectrum lighting to treat these children. This practice was changed in the last 25 years to use artificial spectrums that subtracted out the UV spectrum and the IR spectrum of light. The reasons were based on beliefs of researchers without any knowledge of how both frequencies are protective of normal cell lines in infants. This was done before neuropsin and melanopsin could be studied and controlled for in these studies on children. The neonatologists were just looking for other light options to treat jaundice to fit with their precepts of the truth. This belief system has also pointed modern eye researchers to why unopposed blue light on the skin and eye may be the real pathologic mechanism is melanoma generation.
Further evidence underpinning a link between blue light and UM comes from neonatal blue light therapy studies. Blue light therapy is an essential tool in treating modern neonatal jaundice in neonatal ICU’s because dermal/subcutaneous bilirubin absorbs light maximally at 425–475 nm. Children with jaundice are born to mothers with light mismatches that drove heteroplasmy rates in her maternal germ cell line. This is 100% in the blue range of the visible spectrum of light. Because of this, pediatrician and manufacturers have changes light sources to match the spectrum of bilirubin without ever considering the collateral damage to the infant’s eye or skin. I already mentioned that the young lens allows massive penetration of blue light. It turns out the skin and subcutaneous fat layer of an infant does the same.
Blue light is reflected by bone. Infants have very poor skeletal development so they are very translucent to blue light. When blue light hits bilirubin, it leads to its conversion to a less toxic water-soluble form that the child can clear via the bile and urine. What is not well understood is how blue light stimulates mitosis of melanocytes in children. We know it stimulates them in animal models but this has not been studied on human infants. There are, however, two observations in humans that have been made that can explain what we would see if we studied humans under the strong blue light.
The first is women of childbearing age. The same effect can be seen in women with melasma. They tend to get darkening of their skin in areas where the bone is just below the surface to reflect the blue light. Women in this age group differ from infants in that they are skeletally mature. Melasma tends to occur over the forehead, upper lip and on the cheeks of women and not where dense bone/teeth are present in the face or lip. Data from laser therapy show that blue light is attenuated by bone and teeth as this graph shows in the blue light range.
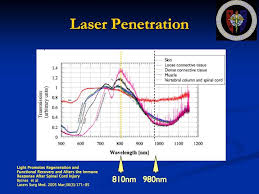
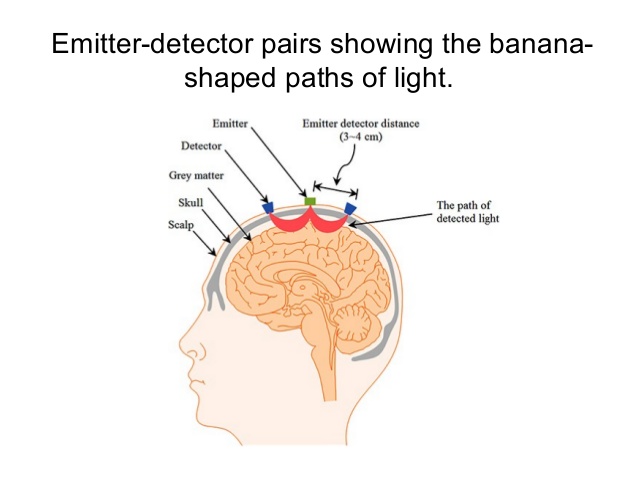
Here you can see below how the skull deflects light frequencies because of its density. We see this in neurosurgery when we try to use IR and NIR light to improve ATP function in traumatic brain injury.
Melasma is often blamed on UV light and hormone changes but this are laughable premise when one considers the graph here and the published data on the effect of UV light on sex steroid hormones.
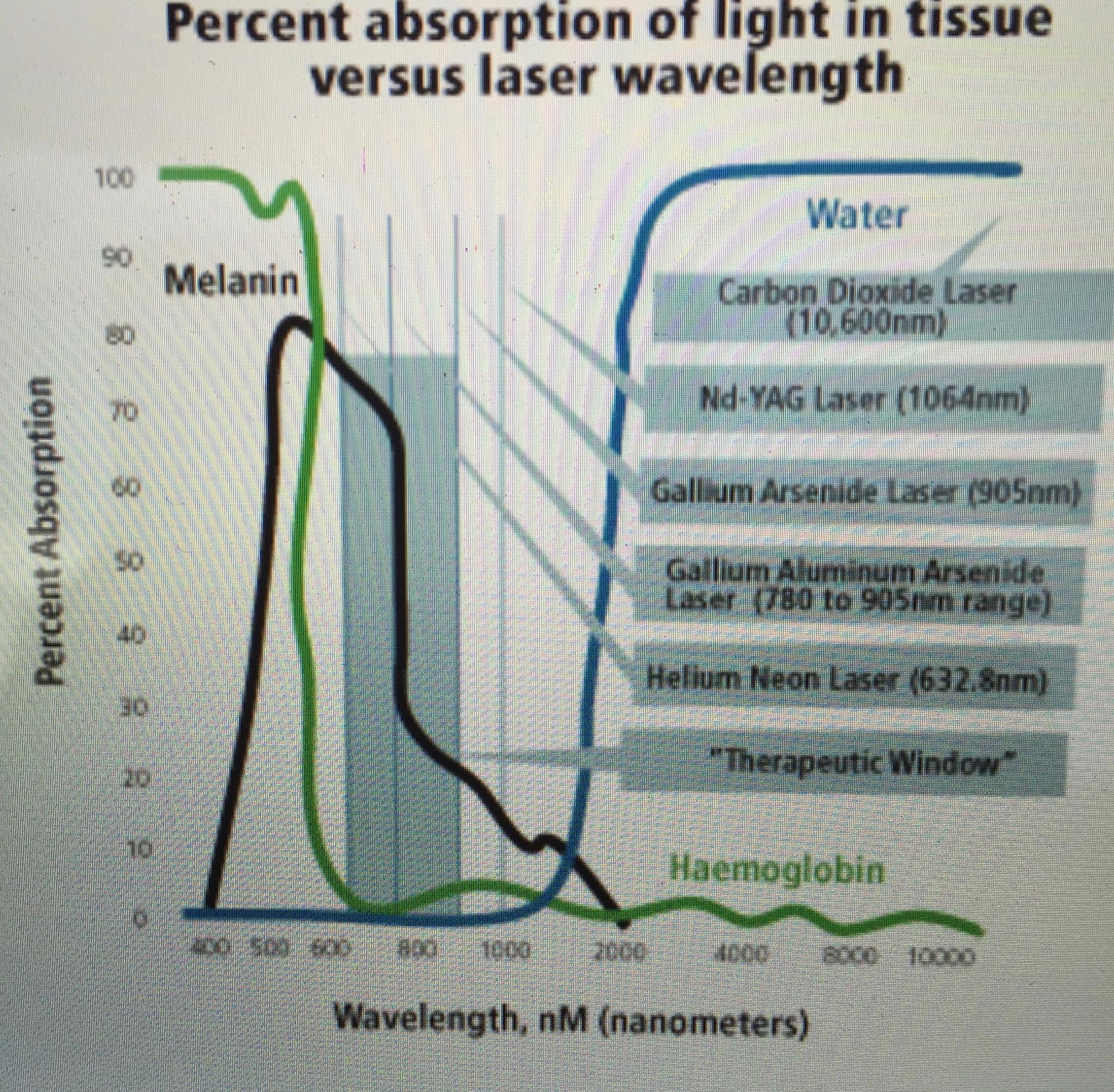
This graph shows that melanin strongly absorbs in the 400-500nm blue part of the spectrum.
Solar UV light and hormones affect all parts of the face in women yet not all parts are effected in melasma. Why is that? The effect should be widespread if the pathology was what modern dermatologist believe. Moreover, UV light is known to break down most of the sex steroids in the skin under sun exposure. UVA and UVB do this naturally in the skin. Blue light actually increases sex steroid release from the human pituitary and avoidance of the sun with facial makeup and sunglasses increase their risk or hormone surges in these areas not allowing the sun to inactivate them because of UV protection in makeup and glasses. Most women report a spike of melasma when they are in artificial lit environments and the condition often worsens when they are pregnant indoors and around the birth of their babies in hospitals.
In infants a reported and published long-term side effect of this therapy is the increased risk of dysplastic nevus development in both the skin and eye (clinically, atypical nevi, or dysplastic nevi, are generally accepted to increase an individual’s risk of melanoma) So this means that blue light increases the mitosis rates of melanocytes to cause pigmentation and certain frequencies of light LIMITS this mitosis. What is the brake for this process in humans? Would you be shocked if I told you it was UV light? Yes, the light modern healthcare blames for skin cancer and melasma.
THE ALPHA MSH/POMC AND ULTRAVIOLET LINK:
When human skin is exposed to sunlight, ultraviolet (UV) radiation stimulates the production and release of a hormone, alpha-melanocyte stimulating hormone, or α-MSH. This hormone is cleaved from POMC which is released by a FULL SPECTRUM sunlight stimulus traveling from the retina to the hypothalamus and pituitary via the central retinal pathways. Alpha-MSH is also secreted by keratinocytes, a specific type of skin cell, then binds to receptors on the surface of another type of cell, called a melanocyte. When α-MSH binds to the receptors, which are known as MC1R, it activates the melanocytes to produce the brown/black pigment melanin in a coupled circadian fashion. When UV light is removed and blue light is present melanogenesis has no coupled feedback control loop. This darkens the tissues with no natural braking mechanism. When this step is blocked heteroplasmy rates in skin cells mitochondria are altered. This is why skin cancer rates are rising in our blue-lit world. Not only are we irradiating our tissues with man-made blue light but we are subtracting the sun’s UV and Ir frequencies. This sets up the perfect storm on the skin. The narrative that sunlight causes cancer in all cases is very suspect because of these findings with how MSH works within the skin with chronic blue light exposure. It would appear a lack of sunlight might be as big a trigger to cancer cases if this step is inhibited in many ways.
The melanin is subsequently transferred back the keratinocytes, increasing the level of melanin within the epidermis, the outer layer of the skin. Humans vary >100-fold in their sensitivity to the harmful effects of ultraviolet radiation. The main determinants of sensitivity are melanin pigmentation and less-well-characterized differences in skin inflammation and repair processes. Pigmentation has a high heritability, but susceptibility to cancers of the skin, a key marker of sun sensitivity, is less heritable because it is related to mitochondrial heteroplasmy rates. Heteroplasmy rates are linked to energy production yield in cells. Melanin is photoprotective to skin cells (protecting them from light/UV radiation) and the greater its density in the epidermis, the more protection is given to the layers of skin below. It does this by absorbing, reflecting and refracting light (particularly UV radiation) and preventing it from penetrating to the nucleus of keratinocytes or to lower levels of the skin. Melanin is also believed to play a role in scavenging free radicals, which can injure skin cells, and in facilitating UV induced apoptosis (programmed cell death), which removes damaged cells. If this step is blocked damage cells cannot be removed and it makes it more likely skin cancer can manifest. It is ironic that the modern narrative might be 180 degrees opposite the teaching in dermatology.
Thus, melanin’s protective role goes way beyond providing a physical barrier. Quantum processes are active protecting us from redox shited mitochondria that are not salvageable and will lead to oncogenesis. It has been suggested that the 2-3 fold melanin levels seen in darker skin types, compared to lighter skin types, convey up to 100-fold difference in sensitivity to ultraviolet radiation due to these protective functions (see Rees 2004).
In addition to activating melanin, α-MSH is known to have several other roles in the skin, although the exact mechanisms are not fully understood. Recent research has shown that α-MSH enhances the repair of DNA damage (such as cyclobutane pyrimidine dimers, or CPDs) a process is known as nucleotide excision repair, or NER – and reduces the generation of free radicals (particularly hydrogen peroxide) following UV radiation impact. Both of these factors reduce the overall damage caused by UV radiation; thus reducing the risk factors for certain skin cancers. One mitigating factor, however, is that α-MSH must be able to bind to the MC1R to achieve this function. HYPERLINK
What can block the binding of alpha-MSH to MC1Receptor?
Clothes, sunblock , contacts, glasses, sunglasses, any mechanical barrier………Now, look at this pic carefully again.
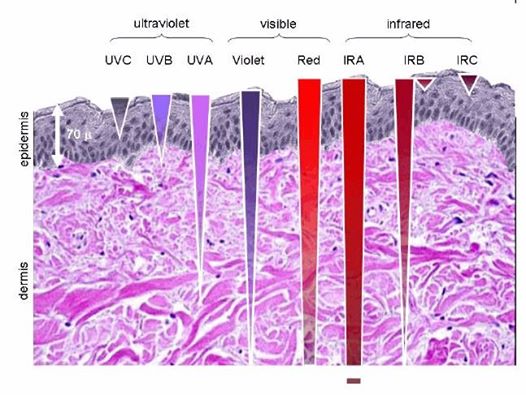
Note that UV light barely breaks the surface, so the blood has to come to the surface to get this irradiation. What chemical is a proxy for this light frequency (UV-A) that does this? Nitric oxide is the answer. It is released from the skin and arterioles under UV-A light stimulus. This explains why we have a UV-A opsin in the cornea and skin. (neuropsin)
The picture below shows you two of life’s main light antenna’s. One is chlorophyll and the other hemoglobin. When you look at their structure you can see how identical they appear. We have proteins in our cells that are light antenna’s to receive this energy and information. My hacks have shown me just how interesting the matter in our cells responds to specific frequency input from the sun. Therefore the matter in our cells is responding to the source in a wireless fashion. Your doctor calls this science biochemistry but calling it biochemistry is a misnomer because we do not understand light well in biology. Biochemistry is really a solid state science of circuits of hydrated carbon-based semiconductors that absorb and emit light that our cells come built with to work with the specific light spectrum of our star and magnetic field on this specific planet.
UV-A only penetrates 1-3 mm, so to get UV light RBC’s have to move toward the surface and they do because of the solar/light nitric oxide couple mechanism. Nature is amazing and our modern beliefs and behaviors are destroying this built-in magic.
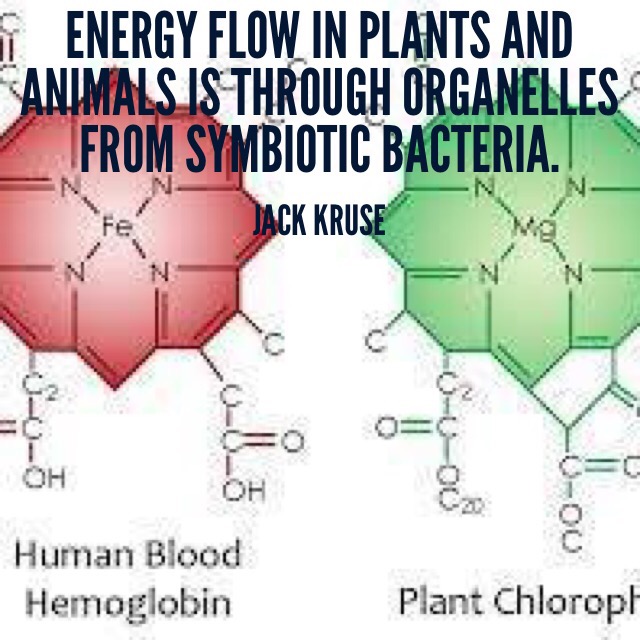
Hemoglobin is a heme protein. Carbon monoxide a byproduct of the heme metabolism. Heme is capable of activating Rev-erb. Rev-erb is a key regulator of circadian cycles. Since heme is an endogenous ligand of rev-erb and heme degrades into bilirubin this implies UV light and blue light are tightly coupled to control the circadian turnover of RBC’s. What is the complementary color of blue? Yellow. Yellow is the color of jaundice in neonates. This is why full spectrum lights are better for neonatal jaundice than the blue lights used today in neonatal units. Blue light irradiation without any corresponding UV or IR-A light will stimulate melanogenesis by cells using the mechanisms mentioned above. Elevated levels of bilirubin cause jaundice in the skin and kernicterus in the brain of a newborn infant born to mother with a circadian mismatch. We use light to photo inactivate bilirubin so the brain is not damaged by jaundice. Modern treatment of neonatal jaundice is now limited to exposure to monochromatic blue light in nurseries. We know that blue light in the AM sun is stimulatory to the anterior pituitary hormones, and POMC and is also a major regulator of circadian rhythms. In fact, rev-erb is an executive-level player in this game. The primary mechanisms of blue light appear unrelated to most people in these two models (melanopsin activation vs. bilirubin photoisomerization step), but to the quantum clinician, they are intertwined by how mitochondria work with light and blood pigments. Our red cell mass turnover is one of the key circadian light signals to the NAD+/NADH couple of cytochrome one that affects mitochondrial DNA biology and this is why the heme degradation pathway activates Rev-erb to couple to the circadian mechanism via NAD+. Is this why people with younger blood seem to stay more healthy in parabiosis studies? Yes it is. How? NAD+ is the key metabolite for circadian chromatin remodeling. NAD+/NADH absorb light at 334, 340, and 365 nm. The hydrogen in NADH is the key to this process. Its spin is of paramount importance.
Look at the picture above again. Chlorophyll and hemoglobin are linked by evolutionary symbiosis and by solar light too. Both are stolen bacteria that cells used to create energy flux in cells using sunlight. Chlorophyll is optimized to blue-green light and hemoglobin is optimized for UV/IR light. Chlorophyll helps plants move toward sunlight because of unique UV phototropic proteins in the leaves. Hemoglobin does the same thing because of nitric oxide and hemoglobin’s absorption spectra.
Sunlight is a stimulus that makes plants and blood vessels move toward its light too. In the skin and eyes, our blood vessels move toward sunlight too because of nitric oxide (NO) release. Sunlight is unpolarized but when it hits our cells it becomes polarized by our hydrated proteins in cells and arterioles. This small change is what releases nitric oxide by electromagnetic forces. Sunlight shifts blood into the skin by changing polarization in tissues that allow for dermal pooling due to molecular resonance changes in endothelial NO synthetase and NO. More than 50% of your blood volume can change your skin surface when specific solar spectral density is present. 60% can pass through your retina in the RPE!!! This can lower your blood pressure by altering renin function via the blood while raising your sulfated vitamin D3, alpha MSH, while lowering your LDL cholesterol level and raising your HDL levels. Sunlight changes the anatomical structure of the molecules in skin cells by changing the optics surface using polarization. It becomes a sensory stimulus for the interoceptive system to induce biochemical substrates via ” a photosynthetic like mechanism”. We see this in plants and now we have proof it alters animal physiology because of measured changes in the mitochondria’s ATPase by using red light and water in animals. The Q-cycle frequency shift light to make red light to change cytochrome functions. This was the topic of my December 2016 webinar for members of my website. Don’t you think it is time to join? Take another look at that picture above.
Chloroplasts and mitochondria both were stolen from a bacteria in the evolutionary past. This entire webinar has been about tracking and linking what human beliefs have been doing to our symbiotic bacteria for the last 150 years. I want you to see it for yourself. Most people are blaming disease on the wrong things in healthcare today. Using our detective skills taught to us by Semmelweis and Snow we can do the same if we become smart detectives to follow the data nature provides. You don’t need an RCT trial to prove it either. Semmelweis and Snow did not use it and solve major medical issues in their day and I believe we can too.
Life is designed to be as predictable as a pair of dice, and this is the very reason why plants and eukaryotes stole a bacteria and turned it into a chloroplast and mitochondria. Both work with excitons to eliminate time as a critical factor in transmutation of light into chemical matter. What does my Reality 1 and 2 blogs teach you about? Excitons. It allowed cells to make better predictions using solar light. Do you still think membership at my site is a waste of time?
Man is a producer of actions because of his neocortex. It is the process of production of thoughts and actions which allows man to alter his environment, to contravene and interfere in the previously external process of evolution to affect change on his environment and for his environment to affect massive change on him. The latter is often underrepresented by medicine and society in general. It is these effects that will define his species next step or how the environment extinguishes his flame. When man began to internalize and ultimately subject the evolutionary process to human control his demise began 700,000 years ago when he invented clothing and blocked the sun from his skin.
Clothes block sunlight to the skin and send the signal of winter year around. While eating carbohydrate out of season, indoor heating, blue light, nnEMF send the signal of perpetual summer and daytime. Our ability to manufacture a comfortable environment filled with alien light and nnEMF is driving neolithic biological chaos. The mind can’t distinguish comfort or convenience from safety because of how the system is built to react. In essence, humans have created an environmental “light hell” for our mitochondria and this hell is where our diseases are coming from.
When you first start on a ‘wellness journey’ you chasing down health issues one by one with this supplement – that protocol etc. With wisdom, you learned that if you change the conditions of existence, this releases the doctor within you and most of the individual problems or symptoms vanish without drugs or supplements. Healthcare becomes cheap.
Clothing = sunscreen = glasses/contacts = sunglasses = smog = air pollution = lowered quantum yield = lowered solar power in all ranges = lowered UV exposure = Earth does not have its full spectrum of light = tarp over a tree = trees dies no matter if it is watered and has access to CO2 and minerals = your modern world modeled.
SUMMARY
Its raining secrets and lies in many fields of medicine and solar science will be the best disinfectant that will cleanse the bad science we believe today in medicine eventually.
Believing that the sun causes melanoma is really becoming akin to “media astroturf”. If you don’t know what that is look up the TED talk on astroturf. The original studies that linked UV light with cancer were all done with isolated UV sources of light. Sunlight is never devoid of its other frequencies and it is now clear from LLLT and mitochondrial medicine that there is a lot of synergy in mitochondrial with all the frequencies in the sunlight that built health and do not destroy it.
I became interested in Vitamin D3 when I became interested in gene regulation. While oncologist has downplayed the effect of D3 levels the literature outside oncology is brisk and in favor it. Molecular biology introduces most MD to genetic determinism in med school and how the genes are regulated. As you know, genes encode the information necessary to build proteins from nucleic acids. Right there that close a link tells you-you need to understand this process well to get a handle on cancers in your patients. For non-scientist readers to understand what that means, one has to take a step back and understand what cells really are. They are collections of hydrated semiconductors that emit LED light in the ELF-UV range. Once you understand this, you start asking the question why are we afraid of UV light if our own cells use it physiologically?
Cells are units of life, filled with hydrate carbon-based polymers of carbon semiconductors. Cells range from simple unicellular organisms to complex multicellular ones like humans. It is helpful to imagine that a cell is like a city or a city-state with multiple zip codes. While proteins contribute to the infrastructure of the cell, they are above all like the specialized individuals who make the city work, with all of the specialized tasks that entail. Some of these jobs (e.g., police, bus drivers) are common to all cities, while certain types of expertise (e.g., specialized types of engineers or scientists) are found only in selected areas of the body. The eye and brain are good examples of zip codes in our bodies.
Similarly, cells in the liver or, say, the brain will produce common proteins while others will be specific to each cell type. Thus, protein production is specific to the function of a given cell to some degree.
All of this means that protein production must be carefully regulated by something. The first and, I believe, most important point of this regulation is the control of the first step: gene transcription of proteins by ubiquitin. Although it is not evident at this point in the oncology conversations in medicine, this is highly relevant to how vitamin D3 works at the molecular level. Sunlight is a powerful chemotherapy for cancer. Cancer regulation in oncology literature always links back to calcium homeostasis or the lack thereof. Vitamin D3 controls this and about 1,000 other human regulatory genes.
When a clinician begins to understand that the active form of vitamin D is four metabolic steps removed from cholesterol in our skin, you have to wonder why evolution put cholesterol and D3 in the same spot where the sun hits them. The physiological effects of vitamin D thus arise through the regulation of gene transcription. Vitamin D was discovered for its capacity to regulate the body’s uptake and use of calcium, in particular, its role in maintaining normal bone health. The problem was medicine thought that bone physiology was the key function of D3 for the last 100 years. It turns out this is untrue.
My interest in vitamin D3 increased when I started to learn about leptin after my knee injury 10-12 years ago. I have a good MD, Ph.D., colleague who mentioned to me something interesting about his work in the lab. He found that the application of active vitamin D3 and its metabolites to cancer cells grown in tissue culture arrested their division. This was eye-opening for me. I never learned about this in medical school at all and when I asked oncologist about this effect must of them were ignorant of it and ignored its impact. I was stunned. Clearly, Vitamin D3 therapeutics could have a massive impact on the practice of oncology with this data. It also pointed out why the artificial light was driving the cancer epidemic. This so-called “non-classical” action of vitamin D became a main focus of my reading because I realized that I could apply my expertise in neuroscience to understand how D3 worked with other hormones like leptin.
I read a paper that made the claim that 3% of the human genome was controlled by D3 and was astounded. No other clinicians I knew even knew this. We now know it controls about 1000 humans genes. That has changed our understanding of vitamin D and health. When I reviewed the epidemiology of cancer and D3 levels in the late 1990’s I found some key links I followed up on. In the late 1990s, there was increasing awareness of the non-classical actions of vitamin D and accumulating population-based studies linking vitamin D deficiency with increased rates of specific types of cancers. However, the molecular details of these actions were completely lacking, so it had NO EFFECT on clinical practice or evidence-based measures. Vitamin D “target” genes showed us that vitamin D3 also controlled the function of the immune system and its primary responses to infection. This was a huge quantum link for me.
Generally one could say that the cathode rays of the sun are generally an immunosuppressant to living things. This is somewhat true of UV-A frequencies but UV-A has been helpful in autoimmune hair loss. Since UVB sunlight creates vitamin D3 from sulfated cholesterol in the skin, vitamin D3 acts as an adjuvant in a vaccine to stimulate activation in the innate immune system. This is why I often call sunlight nature’s natural vaccine program. The active form of vitamin D3 is also capable of increasing superoxide and free radical signaling which can directly combat infections by way of WBC’s. Vitamin D3 is also associated with the creations of collateral immune chemicals called cathelicidins. They are a class of molecules which help the organism to fight bacteria/archaea/viruses. So in a way, our organism uses an inoculation of sunlight to attempt to find an alternative pathway of immune activation. This pathway is useful if the immune system is damaged by another factor or in the short term by an overdosage of infrared or ultraviolet radiation. The endogenous production of D3 in the skin should lead to increased cathelicidin concentrations. Taking oral vitamin D3 ruins this coupled system for tightly coupled immune regulation.
The endogenous Vitamin D3 pathways are still vastly unexplored for infection and autoimmunity prevention, in my opinion. For cancer, the light link on epigenetic expression became obvious when it was clear D3 controlled c-MYC expression. Researchers began to realize that many genes whose transcription was reduced in vitamin D-treated cells were also regulated by a protein called cMYC. cMYC is at the same time similar to the vitamin D receptor and in some ways the opposite of it. It is similar in that, like the receptor, cMYC is a regulator of specific genes’ transcription. However, it is the opposite in the sense that, while vitamin D working through its receptor acts to block cell division, cMYC acts to stimulate it. Not surprisingly, the function of cMYC is elevated in about 50% of all cancers, which are of course diseases of uncontrolled cell division.
Slowly, perhaps too slowly for those with cancer, it dawned on many researchers and clinicians that the (VDR) vitamin D receptor was acting by directly controlling cMYC function. What came as such a surprise to clinical medicine is that vitamin D and the vitamin D receptor control cMYC function by multiple mechanisms. This mechanism is still not well known in medicine if you can believe it. Places like OZ and their use of sunscreen prove it.
The VDR and D3 levels depress the rate of transcription of the gene encoding cMYC and thus the production of new cMYC protein.
In addition, they increase the rate of degradation, or turnover, of existing cMYC protein. Moreover, they have opposite effects on the production and turnover of a protein called MXD1 that antagonizes cMYC function, leading to dramatic swings in the relative amounts of cMYC and MXD1 in vitamin D3-treated cells.
There is a problem with D3 as a therapy as my blog laid out in my Time 11 blog. We currently believe/think that vitamin D’s control of cMYC function is one of the key elements of its capacity to control cell division and we believe that it represents an important aspect of its anticancer properties. Its critical to point out to those with cancer what the data is showing is by using the term “anticancer” and D3 in the same sentence, it means D3 is helpful in the prevention of cancer development, not the treatment of existing cancers. This is why I rail against sunscreen use and sunglasses. They are putting people at risk for cancers, and the September 2016 webinar I did showed the timeline of why I believe it. This is why Jamie Ward felt compelled to ask me to write up the webinar and post it. Today’s post is that write up.
As I hope most of you know now, as cancers progress they can become resistant to various types of therapeutic and chemotherapeutic approaches as heteroplasmy rates become worse, and that is also true with a vitamin D3 treatments offered post-diagnosis. Vitamin D3 gets no exception here but this is not what functional medicine types tell people. I do. This is why I tell people to stop using pills when you have no cancer……..it might lead to cancer because of how D3 works with c-MYC. People who have half the story can make huge errors because they do not understand the non-linear effects of light on mitochondrial biology.
CITES:
http://www.tandfonline.com/doi/full/10.1080/19381980.2016.1248325
http://www.ncbi.nlm.nih.gov/pubmed/19519827/
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4488093/
V. P. Papastefanou and V. M. Cohen, “Uveal melanoma,” Journal of Skin Cancer, vol. 2011, Article ID 573974, 13 pages, 2011.
http://www.museumofvision.org/exhibitions/?key=44&subkey=4&relkey=35
https://www.researchgate.net/publication/228769778_FM_Broadcasting_Exposure_Time_and_Malignant_Melanoma_Incidence
Y. Kuse, K. Ogawa, K. Tsuruma, M. Shimazawa, and H. Hara, “Damage of photoreceptor-derived cells in culture induced by light emitting diode-derived blue light,” Scientific Reports, vol. 4, article 5223, 2014.
J. Oláh, E. Tóth-Molnár, L. Kemény, and Z. Csoma, “Long-term hazards of neonatal blue-light phototherapy,” British Journal of Dermatology, vol. 169, no. 2, pp. 243–249, 2013.
T. Okuno, H. Saito, and J. Ojima, “Evaluation of blue-light hazards from various light sources,” Developments in Ophthalmology, vol. 35, pp. 104–112, 2002.
B. F. Godley, F. A. Shamsi, F. Q. Liang, S. G. Jarrett, S. Davies, and M. Boulton, “Blue light induces mitochondrial DNA damage and free radical production in epithelial cells,” The Journal of Biological Chemistry, vol. 280, no. 22, pp. 21061–21066, 2005.
A. D. Singh and A. Topham, “Incidence of uveal melanoma in the United States: 1973–1997,” Ophthalmology, vol. 110, no. 5, pp. 956–961, 2003.
G. Virgili, G. Gatta, L. Ciccolallo et al., “Incidence of uveal melanoma in Europe,” Ophthalmology, vol. 114, no. 12, pp. 2309–2315, 2007
J. M. Elwood and J. Jopson, “Melanoma and sun exposure: an overview of published studies,” International Journal of Cancer, vol. 73, no. 2, pp. 198–203, 1997.
P. V. Algvere, J. Marshall, and S. Seregard, “Age-related maculopathy and the impact of blue light hazard,” Acta Ophthalmologica Scandinavica, vol. 84, no. 1, pp. 4–15, 2006.
C. P. Shah, E. Weis, M. Lajous, J. A. Shields, and C. L. Shields, “Intermittent and chronic ultraviolet light exposure and uveal melanoma: a meta-analysis,” Ophthalmology, vol. 112, no. 9, pp. 1599–1607, 2005.
M. A. Saornil, “Iris colour and uveal melanoma,” Canadian Journal of Ophthalmology, vol. 39, no. 4, pp. 448–452, 2004.
Z. A. Abdel-Malek, V. B. Swope, R. J. Starner, L. Koikov, P. Cassidy, and S. Leachman, “Melanocortins and the melanocortin 1 receptor, moving translationally towards melanoma prevention,” Archives of Biochemistry and Biophysics, vol. 563, pp. 4–12, 2014.
M. A. Mainster and P. L. Turner, “Ultraviolet-B phototoxicity and hypothetical photomelanomagenesis: intraocular and crystalline lens photoprotection,” American Journal of Ophthalmology, vol. 149, no. 4, pp. 543–549, 2010.
T. Laube, H. Apel, and H.-R. Koch, “Ultraviolet radiation absorption of intraocular lenses,” Ophthalmology, vol. 111, no. 5, pp. 880–885, 2004.
S. Di Cesare, S. Maloney, B. F. Fernandes et al., “The effect of blue light exposure in an ocular melanoma animal model,” Journal of Experimental and Clinical Cancer Research, vol. 28, article 48, 2009.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4389734/