

 READERS SUMMARY:
READERS SUMMARY:
1. WHY ARE VITAMIN D LEVELS REALLY IN RETREAT IN OUR MODERN WORLD?
2. WHY SUPPLEMENTING WITH ORAL VITAMIN D BE PROBLEMATIC FOR SOME?
3. HOW IS NATURAL ACTINO-THERAPY SUPPOSED TO WORK USING NATURE?
Most people know that Vitamin D is made from certain wavelengths of sunlight in the UVB range. I covered that in detail here. Low Vitamin D levels can be caused by three different clinical scenario’s. One is due to low endogenous Vitamin D levels due to a deficiency in sun or in foods with Vitamin D. This is rare today. These cases will have a low vitamin D level with a low to normal calcium level. The second will be a low vitamin D level with a high calcium levels. This is usually due to a parathyroid tumor. This is also rare. Low Vitamin D levels lead many clinicians say: “your vitamin D is low, and your calcium is a little high, I think you may have secondary hyperparathyroidism due to the low vitamin D, so here is a prescription for 10,000 (or 50,000) units of vitamin D. Take this high dose of vitamin D and come back in 3 months and we will check your calcium and vitamin D levels again”.
You’d be surprised how many times those exact words will be said–dozens of times per day in every city of the USA—and it is wrong every time. WHY? Vitamin D is required to absorb calcium from our diet. But Vitamin D3 has several forms in the body that do different things. Sulfated Vitamin D3 is made from specific frequencies of sunlight in the AM that has little to do with calcium homeostasis. Un-sulfated Vitamin D contains the ability to regulate calcium homeostasis in the blood. You should realize a low vitamin D level will cause you to absorb LESS calcium in your gut, not more. It is not the goal of sulfated Vitamin D we get from the sun. This is huge teaching point here. Today’s blog is not about parathyroid tumors, it is about your altered environment. When you cannot use starlight to sulfate your lipids and proteins you do not allow Sulfur or Phosphorus to act like quibits to charge your quantum batteries. Our modern environment makes it appear the sun is a toxin. Nothing could be further from the truth.
Cholesterol and Vitamin D3 are nearly identical in chemical structure. Most people do not know this. Sunlight naturally sulfates these things. The only difference in both bio-molecules is a single double bond in the second ring of the cholesterol backbone. This gives Vitamin D3 one less hydrogen atom than the closed ring of cholesterol. After reading Tensegrity 6 that should make you think a lot more carefully about atomic details. One hydrogen is the only difference at the atomic scale. Here you will see the wisdom of Tensegrity 6 play its role. Hydrogen is the ultimate chameleon for the sulfation and differention of cholesterol and Vitamin D3. What does it do? Vitamin D3 is synthesized from cholesterol in the skin upon exposure to specific frequencies of sunlight. When this happens and calcium is normal in the blood serum, both molecules remain sulfated by melatonin. DON’T FORGET THIS MECHANISM. THIS HYDROGEN INTERACTION WITH and WITHIN THE SUN IS HUGE to maintain sulfation of lipids and proteins. THIS is the basis of how a quantum dot battery is built in animals.
In the recent past, it was taught in medical training that a low vitamin D3 could never be the cause of high blood calcium without a tumor. That was absolutely true until modern technology became prominent in our society. Today it is no longer true. This leads us into the least known etiology of low vitamin D3 levels today that is the most misunderstood. It can be associated with a low, normal, or high calcium level because of a chronic calcium efflux in neurons and glial cells close to the paraventricular nucleus (PVN). When calcium is effluxed inappropriately in mitochondria, it directly affects the amount of sulfate anions in your blood. Sulfate anions are the 4th most common anion in blood. The PVN are the cells in the brainstem that “sense calcium levels” in the blood by way of the hydrogen bonding network in the water of CSF. We lose the ability to sense this as changes in the concentration of electrons and protons in alter CSF.
THE GUT VERSUS THE SKIN
Sulfated vitamin D3 in humans is tied to exposure of UVB sunlight. It is not tied to any gut mediated mechanism, as many dermatologists think. They believe oral Vitamin D3 and solar-derived Vitamin D3 are one and the same. I do not believe they are. The simple oral non-sulfated form of vitamin D likely will not provide the same benefits as the vitamin D created in your skin from sun exposure, because it cannot be converted to vitamin D3 sulfate. Sulfation of vitamin D inactivates it from affecting calcium homeostasis, as the picture above shows. Cite 13 goes into this detail. Sulfated vitamin D3 works differently than oral Vitamin D supplements because sulfated Vitamin D does not resorb calcium in the gut. Sulfated vitamin D3 is made from UVB and IR light and sulfated cholesterol in a very complicated quantum dance. When your skin produces cholesterol sulfate, it vasodilates blood vessels in your skin allowing massive amounts of cholesterol to be bound to sulfate and not having to be bound to LDL made from the liver. If your liver doesn’t have to make so much LDL, the LDL goes down naturally. Your blood pressure also declines naturally. Sulfated vitamin D3 acts as a natural calcium channel blocker in your skin. Calcium channel blockers act to lower blood pressure by increasing proton flows in blood vessels. You can see these effects when you draw labs and know what to look for. When you don’t know what to look for sometimes it leads clinicians to make assumptions about labs panels that make no quantum sense. Rarely are these labs drawn together anymore in clinics. Today, low vitamin D3 is common in people without any other “obvious” health problems, including a parathyroid tumor. Most physicians have no idea why this pandemic is happening, but they know there is a lot of people with low Vitamin D3 for some reason.
 This blog is about “that cause” of low vitamin D3 levels.
This blog is about “that cause” of low vitamin D3 levels.
In my opinion, the modern vitamin D3 pandemic is due to an excessive feedback control from the paraventricular nucleus (PVN) of the brainstem, that forcibly lowers the Vitamin D3 production in the skin irrespective of the sun exposure you get, because of the calcium efflux in the endothelium and blood in the skin. This misunderstanding is due to not fully understanding the “quantum scale” feedback loops in the brain’s PVN help determine how Vitamin D3 is made endogenously from sunlight in our skin and blood plasma. Think of your world without the sun for a moment. Your sleep cycle would normally advance 30 min every day with no sun to signal your circadian rhythms. The modern microwaved life is a world without sun. Without the sun, lipids and proteins go un-sulfated in us, sulfur in your skin, gut, and plasma………..you have no sun even when it rises………how is that for irony. That is a quantum perspective.
Vitamin D is a misnomer. It’s not a vitamin, first of all. Vitamins are supposed to be nitrogen-containing compounds that act as co-enzymes which we get from our diet. We don’t make Vitamin D from food. Some foods have Vitamin D, but those foods are rare. We make it from a specific wavelength of sunlight at a specific time of day. It appears sulfated vitamin D3 and cholesterol have a specific circadian cycle while un-sulfated vitamin D and cholesterol do not. Moreover, vitamin D does not contain nitrogen for a specific reason.
With sun exposure, eNOS provides the nitrogen as mentioned above. Vitamin A, C, and E don’t have nitrogen either, but unlike Vitamin C and E, it is also not a co-factor in humans. It does, however, interact with DHA and Vitamin A via the RXR receptors in the brain.
Vitamin A known as retinol acts as a co-factor by being a precursor of a co-factor in the eye photoreceptor enzymes. When vitamin D3 levels fall, Vitamin A becomes unbalanced in tissues. All opsins in humans are loosely bound to retinol. When retinol is liberated from opsins it becomes toxic and destroys all photoreceptor proteins in humans. When free Vitamin A levels rise in tissues, damage ensues. For example, with blue light exposure of the skin, inflammatory skin conditions and cancers in neuroectodermal tissues are the usual results. The most interesting link is higher VItamin A levels in neuroepithelium also lowers sulfated cholesterol in these cells. Vitamin A is tightly coupled to Vitamin D and DHA levels in the body for this reason. Vitamin A also gets processed in a controlled manner into hormones for other parts of the body.
Vitamin D acts just like a hormone would, by raising blood calcium levels and helping cell differentiation across the body. But unlike Vitamin A’s hormonal form, called the retinoic acids, every other hormone’s production is not produced on demand by homeostatic mechanisms in the body. Vitamin D is not. We need the sun to get it.
Sunlight is the great determinant of how much vitamin D3 you create. Ask yourself this, why on earth would we want sunlight exposure to raise our calcium levels? Much less, to be necessary for absorbing calcium from our food?
GET READY FOR A BOOM:
Calcium efflux lowers sulfate levels in all cells, but especially the skin and surface arterioles where the sun hits us. This ties the mechanism of calcium efflux in the central nervous system to an alteration of blood chemistry in a circadian fashion. This chronic effluxing of calcium seriously disturbs calcium levels, PTH levels, and Vitamin D homeostasis in the skin. This mechanism is tied to sulfation and eNOS in the skin and surface arterial system. eNOS stimulates nitric oxide from L- Arginine and it stimulates sulfate production from sulfur in the presence of UVB and IR light. eNOS switches to nitrate synthesis and away from sulfate synthesis when calcium efflux occurs due to circadian damage.
Calcium efflux also depletes cholesterol from the RBC cell membrane allowing eNOS to change its function via the action of hydrogen’s ability to change how it works in this emergent environment.
- Cholesterol sulfate collects around exterior of red blood cells and gives them a negative charge field. This keeps the RBC’s from clumping together or sticking to capillary walls. It also helps keep the RBC’s from falling apart when they are deformed in a vessel. Since the sulfated cholesterol is water soluble it can travel freely in plasma and go from cell to cell without any input of energy. (Cite 13)
When calcium levels are altered in the CSF and the blood, cholesterol in the basal skin and blood plasma cannot be sulfated from cysteine stores. The cysteine stores use vitamin B12 which fits perfectly with nNOS hydrophilic heme pocket. It then binds some glutathione from the RBC in the plasma. Glutathione has the ability to carry an extra sulfur atom in the form of GSSH. You might remember, I made that point in Energy and Epigenetics 12. I asked you in that blog, was your battery charged? Little did you know then, I was showing you that your skin is a giant solar powered battery to make sulfated proteins in the arterioles of your skin. In many ways, this sulfated version of cholesterol and Vitamin D3 perform the same functions of chlorophyll in plants. These proteins are designed to diffuse sunlight and help you retain water while absorbing on the specific wavelengths of light that cholesterol and Vitamin D need to keep you well. When you do not get those frequencies all quantum hell breaks loose because of calcium efflux. I cannot stress to you how big a deal this is.
KEY POINT: In summer, we use eNOS with the photons of UVB and IR light to make sulfated proteins to deliver cholesterol and oxygen to tissues that need it. In winter, we use eNOS to deliver cholesterol and oxygen to tissues that need it using a plasma that is more loaded with electrons. Here you can see how our SCN goes from its light switch to its cold switch that I mentioned in CT 4 and CT 6. This is the metabolic trap door of the Ancient Pathway. Calcium efflux is the key metric to the change in the metabolic sensor in seasons. Today’s technology alters how that switch works.
The higher calcium levels decrease cholesterol in the RBC to make it leak some glutathione for this reaction to happen. Within the heme cavity lies two zinc atoms which draw this “extra sulfur” into the pocket to interact with eNOS, two flavin proteins, BH4, and electrons from sunlight in two specific frequencies. This turns superoxide made from eNOS into sulfate. The flavin proteins (and BH4) give up electrons when they interact with sunlight. Sulfate has to balance with K+ ions in cells when calcium is effluxed and cholesterol is depleted in RBC’s. This links to Ling’s work from the 1950’s that science has ignored. Ca2+ has to be balanced by NO3– to maintain balance. When you lose this balance you affect the solubility of protein polymers in us. Along with the redox potential of the cell, this balance maintain order inside the water protein structure of the cell.
In other words, protein folding machinery fails and cell can no longer synthesize the correct size and shape proteins. This creates the thermodynamic problem I mentioned in blog’s OSF3-5. When you screw this up you need to replace your proteins using ubiquination. This costs a cell a lot of energy.
These ideas come directly from Gilbert Ling’s, Albert Szent Gyorgyi, and Stanley Prusiner’s work. This is why this blog could not come earlier in the Quilt. You needed a lot of back ground info to fully understand the details. The October 2014 webinar kicked open this door. This blog fills the room with the light of wisdom.
WHY IS THIS BIG?
When calcium is effluxed for any reason, (non native EMF #1 cause today), cells immediately switch from making sulfate in surface blood vessels to nitrate synthesis. So sulfate levels drop everywhere. This directly affects Vitamin D 3 and cholesterol function, as you will soon see. Neither can be sulfated as they normally would be, even when the sun is shining brightly. This is why dermatologist believe the sun is bad when it is not. The reason is because we can’t make sulfate in our skin when the sun hits it. This is the perfect storm we face in our modern world.
Sulfur stores ultimately come from things I mentioned in the EPCOT Rx, Energy and Epigenetics 12, seafood and pork. Cholesterol sulfate is manufactured by a combination of specific frequencies of
(1) ultraviolet radiation
(2) visible light radiation
(3) infrared radiation
(4) and a specific range of oxygen saturation in our blood
The sulfate actually comes from homocysteine recycling that occurs within RBC’s hemoglobin in the surface arterioles in our skin. This is why elevated homocysteine and low vitamin D levels are a non specific risk factors for heart disease and stroke. Homocysteine is the source of sulfate. You have to consume “some energy” to produce a sulfate from homocysteine, and the red blood cells actually supply the ATP to the plaque. ATP withdraws electrons from homocysteine to sulfate the cholesterol in blood. Many people forget that RBC have no nuclei or mitochondria so you might be wondering where the ATP comes from? Because of the lack of nuclei and mitochondria, mature red blood cells are incapable of generating energy via the Krebs cycle. Instead, erythrocytes depend on the anaerobic conversion of glucose by the Embden-Meyerhof pathway for the generation and storage of high-energy phosphates. This is why you can never lower your HbA1C to zero even on a zero carb diet. We need some endogenous glucose production in RBC’s to make small amounts of ATP to move electrons.
BIOLOGY GEEKS: Moreover, erythrocytes possess a unique glycolytic bypass for the production of 2,3-bisphosphoglycerate (2,3-DPG), the Rapoport-Luebering shunt. This shunt bypasses the phosphoglycerate kinase (PGK) step and accounts for the synthesis and regulation of 2,3-DPG levels that decrease hemoglobin’s affinity for oxygen. This works in concert with the magnetic flux forces that allow paramagnetic diatomic oxygen to be drawn to mitochondria. In this way, 2,3-DPG constitutes a quantum energy buffer to catalyze this reaction. This frees sulfate to bind with cholesterol in blood plasma. When your LDL cholesterol is elevated, it is a sign your skin is lacking sunlight in these specific frequencies. These frequencies occur 9-12 noon in most places on the globe. Why is this pathway critical from a quantum scale? Oxygen transport in blood is dangerous game for life. The sulfate molecule supports safe transport of O2 in blood. Nitrogen makes it much more dangerous. Cholesterol depletion in cell membranes forces cells to switch to nitrogen-based O2 transport. Normally, this only occurs in the absence of sunlight in winter. In our modern environment, it happens 24/7 while people eat a carbohydrate diet 24/7. This creates a huge problem for mitochondria.
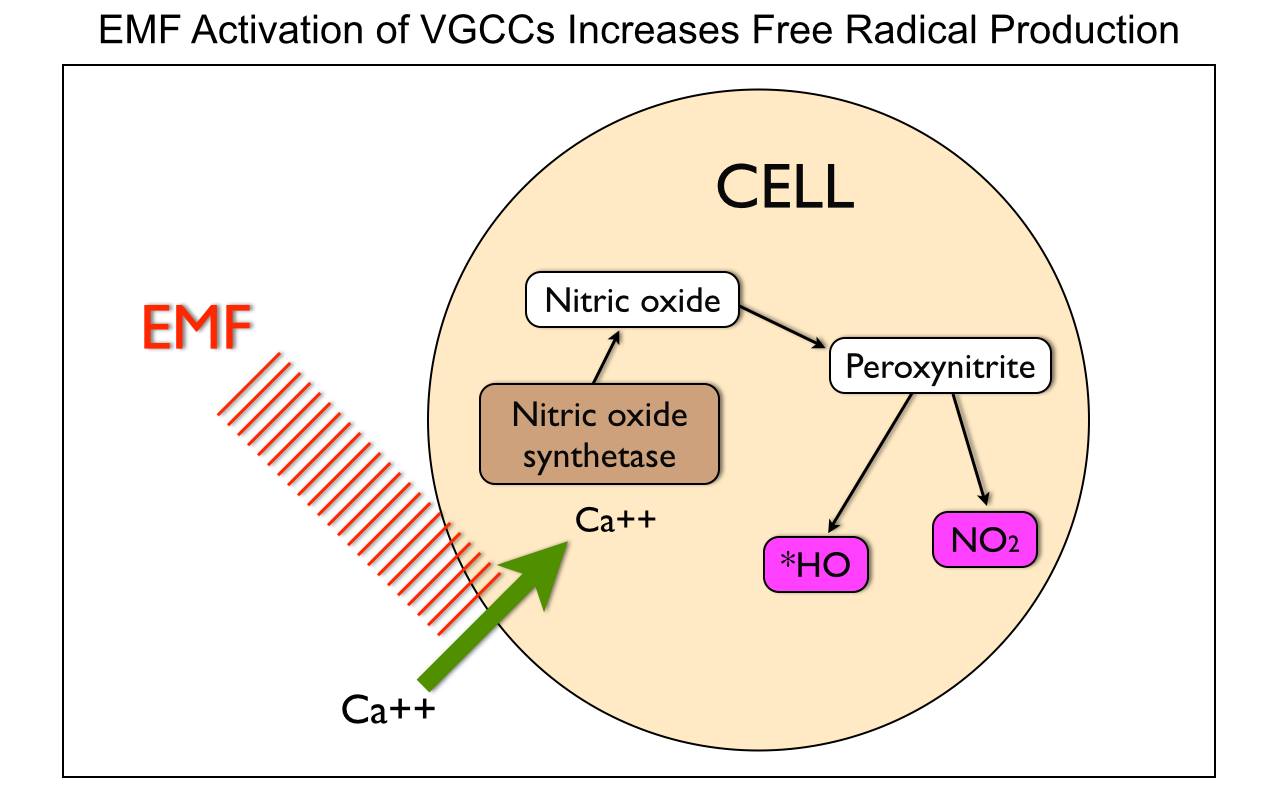
Both systems preserve the paramagnetic status of diatomic oxygen. Calcium efflux forces eNOS to synthesize NO instead of sulfate in blood and endothelial cells. This single atomic change alters the movement of electrons in blood and endothelial cells. These electrons carry the sun’s photon energies and information. This leads to widespread damage to cell proteins and fats due to reactive nitrogen species like peroxynitrite when electrons are depleted in the blood plasma or when we are dehydrated and calcium is effluxed in the brain. This things happen when we use non native EMF. Non native EMF creates calcium efflux which creates an imbalance between chaotropes and kosmotropes results in protein mis-folding. Once you proteins change sunlight can no longer interact with them the way they were designed by lady evolution. BOOM.
When you sulfate cholesterol, you turn it into a water-soluble chemical. This allows it to become a solvent in blood plasma. This allows it to get into places using water’s piezoelectric and superconducting proton cabling systems in cells you recently learned about. Cholesterol doesn’t have to be packaged up inside a low-density lipoprotein (LDL) particle made in the liver to be used by cells. LDL production in the liver is a sign your environment is badly altered. When sunlight interacts with eNOS and cholesterol some quantum magic happens in skin.
Most biologic cell membranes in skin give no intrinsic Electron Paramagnetic Resonance (EPR) signal because they normally have no unpaired electrons. However, when the skin is affected by certain frequencies of sunlight unpaired electrons show up in droves. This occurs because eNOS is used to make cholesterol sulfate normally. Anytime a nitroxide molecule is bound to a macromolecule it becomes a type of electron spin label we can look for in experiments. Becker used this technique in his work to monitor electron spins using a spectrometer to see the effect (EPR). Lady Evolution uses nitric oxide as an intermediate in this process and is the key to making cholesterol stay paramagnetic. Anything that is paramagnetic is drawn to tissues with a large magnetic field. It tracks to tissues with mitochondrial density. This is also why O2 transport is tied to paramagnetism of diatomic oxygen. Unpaired electrons do show up in sulfated cholesterol because of the quantum action of UV sunlight on the sulfur and nitrogen atom. Sulfated cholesterol becomes paramagnetic under the direction of sunlight. This is how cholesterol works in a quantum fashion, and how it is delivered to tissues naturally. This is why high LDL cholesterol can be used as a marker of a bad environment. It also causes pregnenolone steal syndrome. Few people realize how important the sun is in biophysics. What modern clinicians do not realize is how our proteins are altered by calcium efflux. The sun is not the bad guy, but modern technology makes it appear that way. I’m betting they will eventually get this correct when the scale the science to my level.
In fact, Vitamin D3 also triggers cellular changes that are necessary for the absorption of magnesium, iron, zinc and phosphate too.
This means the solar frequencies are incredibly specific in their actions and important to biologic construction at an atomic level for some reason.
In our evolutionary past, before clothes and civilization, we may have always gotten enough UV light on our skin to create the proper pro-hormones, but what about nocturnal or burrowing mammals?
It seems odd to have a hormone, that is necessary for key nutrient absorption and dependent on exogenous factors that seem to have nothing to do with the hormones function. This oddity is only weird when you have biologic glasses on. It makes perfect sense at the biophysical scale, where light and proteins interact.
Today, those low in Vitamin D3 think taking an oral supplement is as good as being in the sun. Dermatologist also believe this. This is also not true, in my opinion, if you read the old research on Vitamin D. Bicknell and Prescott found in 1953 in their exhaustive research that that “sunlight acting directly on the body should be the way in which Vitamin D is obtained”. They found in their research that the gut and body have have no power to regulate the amount of vitamin D it absorbs from food. Foods rarely have Vitamin D3, so from an evolutionary perspective this is not a big issue. This is likely why there is no gut feedback. Today, most humans low in Vitamin D, are now relying on their gut to supplement Vitamin D because they are not getting any sun. That implies we might want to be careful about what we are doing today to treat low Vitamin D levels with an oral supplement.
This means taking vitamin D orally has no true negative feedback control normally. Oral vitamin D will still help increase your plasma levels but this may not be what you want to do until you understand why you vitamin D level is low to begin with in today’s world.
This implies if there is another reason that calcium levels are raised artificially, the body will react by lowering its endogenous production of Vitamin D. It raises an interesting point, could it be this is why modern man faces an epidemic of low Vitamin D levels? It also points out why taking a ton of oral vitamin D may not be ideal, if this is the case. I told people in CPC #9 that if our body makes it you probably should not be supplementing it unless you understand the scale and context of the clinical problem. In today’s world, that is very accurate with respect to Vitamin D3. Why?
If your species has created an environment that chronically causes efluxing calcium from neurons, glial cells and your skin, taking exogenous Vitamin D3 could lead to cardiac instability. Calcium controls the depolarization in the atria and ventricles of our heart. Today we are seeing epidemic levels of atrial fibrillation with low levels of Vitamin D and no one seems to connect the dots. People with high calcium levels are also know to have increased pain. Many pain specialists are using calcium channel blockers to treat these patients. Today we are seeing massive amounts of patients with chronic pain in all specialties. The symptoms of calcium deficiency blend so well into our everyday lives that they often go unnoticed or at least don’t set off any alarms for greater attention. Calcium acts as a natural tranquilizer in our bodies by altering depolarization of sensory nerves. Neurosurgeons know this. It has a calming effect on our nerves which in turn has a calming effect on our muscles helping to reduce chronic pain. Many believe that altered calcium homeostasis is tied to chronic fatigue, mental illness, ADHD, and fibromyalgia. I do too.
What most people do not know about Vitamin D is that the main feedback loop that controls its action is on blood levels of calcium that the brain stem senses through N- type calcium channels. The blood levels are directly tied to loss of intracellular calcium. Non native EMF’s like blue light, causes this chronic calcium efflux. Nora Volkow’s research work has expertly shown this effect in detail. It’s time you connect the dots.
This implies that Vitamin D levels that stay low today, are a sign of a very altered environment that we live in. Vitamin D normally raises calcium resorption in the gut and raises calcium in the blood. Blood calcium levels are the predominant negative feedback control of how much or little Vitamin D3 is made in our body in the skin. You might recall from Energy and Epigenetics 3 and 4, that non native EMF major effect on cellular metabolism is calcium efflux. Taking oral Vitamin D3 may raise your calcium levels to dangerous levels and affect CSF in the brain and signaling in the PVN. The most common clinical sign this is happening is a low magnesium level associated with a high BUN/creatine ration, with the presence of heart rhythm abnormalities, and kidney stones.
NEUROSURGERY GEEKS: N-type calcium channels have been recognized as key targets in controlling pain through modulation of the entry of calcium into neurons. When a pain signal is initiated, calcium channels open and the influx of calcium ions trigger the release of neurotransmitters, which thereby potentiates the signal to the brain where it is perceived as pain. This pathway has been targeted and clinically validated by a commercialized product called ziconotide (Prialt), a peptide N-type calcium channel blocker that must be administered directly into the spinal cord. When [Ca2+]ECF is too low (hypocalcemia), voltage-gated ion channels start opening spontaneously, causing nerve and muscle cells to become hyperactive. These changes are driven by glutamate channels and quelled by nitric oxide. Today people complain of muscle spasm chronically. Pain physicians are reporting record numbers of patients with fibromyalgia and no one knows what to do with them? The syndrome of involuntary muscle spasms due to low [Ca2+]ECF is called hypocalcemic tetany. Conversely, when [Ca2+]ECF is too high (hypercalcemia), voltage-gated ion channels don’t open as easily, and there is depressed nervous system function. This is why mental illness is spiking in today’s world, in my opinion. Non native EMF causes these voltage gated channels to work improperly depending upon the environment the person is in. Another problem of hypercalcemia is that calcium can combine with phosphate ions, forming deposits of calcium phosphate (stones) in blood vessels and in the kidneys. Atherosclerosis and kidney stones therefore are signs that one should look at their environment before consider other ideas of causation.
The neuromuscular symptoms of hypercalcemia are caused by a negative bathmotropic effect due to the increased interaction of calcium with sodium channels. Positive bathmotropic effects increase the response of muscle to stimulation, whereas negative bathmotropic effects decrease the response of muscle to stimulation. A negative bathmotropic effect cause the heart to be less responsive to catecholaminergic drugs released in excess from the paraventricular nucleus in the brainstem. PVN stimulation is caused by calcium efflux and also causes adrenal fatigue.
This implies that adrenal fatigue maybe a protective reaction of the brainstem for the cardiac muscle to prevent arrhythmia’s. It also points out why I am not a fan of using exogenous hydrocortisone to treat adrenal fatigue when it is clear the real problem is an environmental overexposure of non native EMF.
Conditions that decrease bathmotropy are hypoxia or hypercarbia (elevated CO2). Remember oxygenated blood is paramagnetic and this helps mitochondrial function. Hypoxic blood does not deliver DHA and oxygen to tissues that need it. This means that chronic hypercarbia destroys electron currents and the resultant magnetic sense in mitochondria from an energy standpoint. Recall that any current of flow has an associate magnetic force with it at 90 degrees.
BEN GREENFIELD GEEKS: High calcium levels diminish magnetic flux forces because electron currents drop within the mitochondria while we lose cholesterol in our cell membranes; this leads to many complex biochemical steps that all lead to the chronic elevation of calcium in the wrong parts of a cell. This all leads to chronic hypoxia. Hypoxia slows ECT transport and up-regulates AMPK pathways and carbohydrate metabolism through cytochrome 1 to generate superoxide. This means electrons from foods will have to enter cytochrome 1. Why is this important? Superoxide is how we signal to make new and better mitochondria. This also depletes us of iodine body wide. This has a really bad effect on the MINOS water shell around our mitochondria. Superoxide is the key signal in mitochondrial biogenesis and in autophagic recycling. It is dampened when iodine is depleted because superoxide is not being made well. Without this ability you lose the ability to recycle your badly functioning mitochondria. When your redox potential is decent, as Ben’s is, you won’t have to worry about fertility, but you will have horrible labs and trashed hormone panels. If your redox potential is trashed because your mitochondria cannot recycle you will be infertile. AMPK regulates PGC 1 alpha, which is also a signal to set off mitochondrial biogenesis. But the central link, the activation of AMKP, is to do one thing: make a mitochondria generate a superoxide signal. This makes it is a self sustaining Rayleigh–Bénard convection loop.
JIMMY MOORE GEEKS: Chronic elevated blood sugars induces something called the Crabtree effect. This mechanism down regulates mitochondrial biogenesis and is linked to a chronically low Vitamin D status. The Crabtree effect chronically can lead to a permanent state of low sex steroid hormones and infertility. This is a sign of mitochondria that cannot make any superoxide and have to rely only on ketone derived acetyl-CoA. This is a really bad place to be and is a big sign you are not healthy when you tell the world you are, because your environment is TOXIC with non native EMF. It also ends in a dead end street littered with no ability for mitochondrial repair or for proper electron transport chain function. The end result on a macroscopic biochemical level is phosphorylation of the pyruvate dehydrogenase complex in mitochondria. This shutters ALL input to the Kreb cycle from glucose. It leaves you with the sense you cannot eat carbs at all, otherwise your health goes to shit further. Mind you, this is actually a false belief, when reality is, it is your TOXIC environment driving the action on ECT! Oh the irony. If you keep missing the boat, on the scale of actions occurring on your neurons, eventually you become unable to even use lactate as a back up system, and you will still get ill eating a high fat low carb diet. That is not good news for many of you , I know. You become left with the belief you must sustain yourself with nutritional ketosis because you can only access ECT via ketone derived acetyl-CoA inputs to the mitochondria. Why is this a bad place to be? Because although the ketones help in the short term…….the electrons are entering an electron chain transporter that is functional DESTROYED and impotent to innovate health or reverse any disease. You will stand still for a long time. When you have bad mitochondria mother nature wont let you procreate. It is kind of a fundamental thing. Have I mentioned that infertility is now runaway everywhere on our planet? Now you know why.
MODERN REALITY: When these things occur in unison on your mitochondria or cell membanes what happens? DHA cannot be delivered to tissues that need it because it is paramagnetic. If DHA isn’t present we lose the electric charge and the associated magnetic force in our mitochondria. People with this issue lose the ability to change sunlight frequencies signals into electric signals. So that they can change native EMF into electrical signals and back to light in other places within cells. When this situation occurs chronically, circadian signaling is further destroyed within the CNS and within cell membranes system wide and significant disease results.
The less ideal your mitochondria hold their electric charges, the higher the fat version your diet has to be to deal with high levels of Ca2+ efflux. As your environment changes and Ca2+ efflux slows, mitochondrial function improves, the lower the fat content needs to be and proteins can rise in your dietary template; as the environments improves further and less calcium is effluxed, your mitochondrial function improves further, the protein levels in your diet should naturally decrease because your ubiquination pathways improve so you don’t not need to replace a lot of protein in your tissues. Modern research has pointed out that people who are big time exerciser’s don’t need a lot of dietary protein. As you improve further, you begin to be able to exercise more, building your muscle mass as well, and then you can add “seasonal carbs” back to your template with out risk. This all assumes that you stop effluxing calcium, of course…………..and today that situation is now very rare. We are created for uniqueness and we are quantum beings living in a synthetic world. What else does all this imply?
FAILEO? It is also well known that low Vitamin D states also raises blood glucose, naturally. That should raise your eyebrow. Might it be why ancestral health pushes the carbs to their followers today? Yep. In fact, Pincussen found in 1937 that carbohydrate metabolism is greatly influenced by ultra-violet and infrared sunlight in combination. The effect is lost when the two forms of electromagnetic energy is delivered separately by artificial means. We have known about this stuff for close to a 100 years but few people are connecting any dots because they do not see the scale of the science. Sunlight is a quantum recipe, not a biochemical one. These forms of sunlight are both coupled in natural sunlight and act to lower blood sugar naturally. Remember, you need DHA and sulfate cholesterol in cell membranes to turn sunlight into an electrical signal in the base levels of collagen to make sulfated Vitamin D3. This points out why strong sunlight in spring and summer helps offset the blood sugar raising effects of foods that grow during these seasons. Nature couples these effects of sunlight on food to limit RBC and WBC glycation. Today these things are uncoupled in modern humans by our choices. RBC and WBC glycation make these cells less paramagnetic and more dimagnetic. When this occurs they cannot deliver their payload of DHA and oxygen as they do normally. The affect of glycation alters the iron oxidation state making the hemoglobin more dimagnetic. Any chemical that is dimagnetic avoids even a decent working mitochondria.
When something is dimagnetic it repels the magnetic field created by a mitochondria. Oxyhemoglobin differs in it’s magnetic properties from deoxyhemoglobin. Oxyhemoglobin is normally diamagnetic like water and cellular tissue. The irony is that the oxygen it carries is quite paramagnetic.
This makes oxyhemoglobin polar magnetic, meaning it has a north and south pole. The O2 bound to it, is drawn to external magnetic fields while the oxygenated heme molecule itself repels them. This makes delivery of O2 easy from an energy standpoint because it is using magnetic flux power to complete the task. The O2 is drawn to tissues with high mitochondrial density because mitochondria have extensive electric currents that generate a magnetic fields and they draw paramagnetic substance to them. Moreover, mitochondria all have an ATPase with an Fo head that generates a magnetic field naturally because it rotates while protons and electrons are moving through it creating Lorentz magnetic forces. This is why oxygen is dropped off in tissues at a fundamental level.
Deoxyhemoglobin is more paramagnetic. The reason for this is its main goal is to be drawn back to the heart’s massive magnetic power because of all the magnetic forces tied to the electrical currents in the heart’s massive capacity of mitochondria to rebind with oxygen delivered from the lungs. This magnetic flux helps offset the pump pressures in the heart. This means deoxyhemoglobin will also be drawn to mitochondria that are making reduced O2. This also helps aid tissue deliver of O2. In neurosurgery, we use functional MRI and the paramagnetic signal of deoxyhemoglobin to delineate tissues well because it produces a stronger magnetic resonance interaction in our scans.
In addition, increased glycosylation of hemoglobin increases its affinity for oxygen, therefore preventing its release at the tissue level and inducing a level of hypoxia in chronic or extreme cases. This is why diabetes is devastating at the local level and why oxygen delivery is altered in diabetes. Diabetics also suffer from another major effect besides poor superoxide levels. They tend to have very low levels of sulfated Vitamin D3 naturally. Why? They are usually blue light toxic and they rarely are out in normal sunlight to harness the UV and IR powers in sunlight. Food exacerbates the diabetic person, but a lack of sunlight and too much fake light are behind why it really happens.
Most people are of the belief that ingesting Vitamin D and getting it from the sun are equivalent. This is not true if your environment is altered. It is really bad if your environment is altered and your gut microbiome is simplified. Today, most humans have an altered flora because of where they live. Oral vitamin D3 does not have the same powerful effect as sunlight in this case because the prokaryotes in our gut are designed to release UV and IR light to our gut enterocytes to activate the Vitamin D receptor in our gut. When the microbiome is altered it does not happen. This means we must rely on our skin to do the job correctly. The only way skin can carry out this task is to have DHA and sulfated cholesterol to turn sunlight frequencies into electric signals in the base of the skin. As you saw above, bad mitochondria cannot deliver DHA to the skin to do this.
WHY MOTHER NATURE ROCKS: The sunlight on the skin cause a vasodilation while oral vitamin D does not. We call this sunburn. This vasodilation allows UV and IR radiations to enter the blood plasma to cause a small but important hemopoetic effect. This hemopoetic effect of UV light is very similar to the effects of we see with higher testosterone or erythropoetin levels in the plasma. Testosterone circadian cycle also is designed to peak during sunlight hours 9AM −12 noon to increase RBC’s mass when UV and IR light are strong. Women’s progesterone levels increase at the same time to increase water density in their plasma. The differences in men and women are subtle but the effects are all tied to the powering up our blood plasma using the 3 legged stool to our advantage. This is why nocturia in both sexes are associated with poor sex steroid circadian cycling. When you get up to urinate at night you cannot sleep well and this alters AM releases of sex steroids that wont see the correct dosage of sunlight to activate plasma/RBC’s/WBC’s. The time of day has the correct dose of UVB and IR light we need to make the quantum dance work. People seem to be missing these fundamental clues to how cyclic coupling in us works. Kovacs (1937) and Barer and Fowler (1945) found with carefully controlled experiments that sunlight caused increases in RBC’s, lymphocytes, and PMN’s. As white cells rise so does the immune system function. UV light is a known natural bactericidal at very specific frequencies and wavelengths that are common to AM morning light.
Before antibiotics for tuberculosis, UV light therapy was used as the treatment for TB. There is a narrow range for the positive effects of UV light on WBC’s so artificial actinic therapy can drop WBC’s and alter immunity. We are designed to get that natural effect from morning-noon sunlight. Circadian biology controls this effect, not your food. Today, it is destroyed in all modern humans. Re-look at Cold Thermogenesis 7 to see how a normal day’s circadian biology should work.
SUMMARY
Generally UV light can raise the zeta potential of blood plasma and water’s hydrogen bonding network. Zeta potential is a scientific term for electrokinetic potential. The zeta potential force might be electric, pressure gradient, concentration gradient, or gravity. Astronauts lose their zeta potential just being in space off our planet. You don’t realize that modern humans also lose it, being disconnected from Earth even one inch above it or when they wear clothing. The further you go away from the planet surface the worse it gets. When you couple this to an ionosphere loaded with microwave energies you have the perfect storm for a pandemic of low sulfated vitamin D3 in humans. For this blog, the zeta potential is tied to RBC’s cell membranes that turn sunlight into an electric signal in blood. When the zeta potential is lower less ATP can be made to sulfate vitamin D and cholesterol. Recall the zeta potential is how much power is stored in electrons in blood plasma. This can be raised by exciting electrons in blood plasma with photons from the sun’s light. It can also be lowered by loss of photons or electrons from the blood plasma. These effects were studied by Eidinow from 1925-34 after Einstein won the Nobel Prize for the photoelectric effect. Sunlight also has infrared light and this acts to lower our blood pressure by increasing proton flows in arteries, provided the arteries are hydrophilic and their walls are at ideal distances from one another. Today we see millions of people with hypertension, and no one seems to know why? Chronically this symptom leads to heart disease and stroke. Both are top killers in modern humans. It is not fat or carbs in your diet causing this folks!
Arteries are hydrophilic when they are preloaded with electrons while protons flow freely within the plasma because of Dr. Gerald Pollack’s work and the Grotthuss mechanism working in unison. The Grotthuss mechanism describes the way protons rapidly move through water to carry more energy. Sunlight powers both of these things naturally with minimal energy needed from the RBC’s ATP. Biology is missing these links in a big way.
You need to be aware of the state of science today. Physics is infinitely deep while biology is infinitely complex, where they meet is where your life comes from. Biophysics is the scale where the life sciences must head.
Since calcium blocks sodium channels and inhibits depolarization of nerve and muscle fibers, increased calcium levels raises the threshold for depolarization in all excitable tissues. Remember the most excitable parts of neurons are in synapses where mitochondria act as permanent magnets to drive magnetic flux and electric currents to facilitate neurotransmitter release. Altered calcium levels slow neurotransmitter release and also diminish neurologic function. Altered calcium levels from non native EMF are directly tied to circadian mismatches of any cause. Few people realize this link today, but it is time you must. It is the number one cause of low sulfated Vitamin D3 and altered cell membrane physiology levels in man today. Your brain is trying to protect you from something you love, but you cannot perceive. You brain is lowering your vitamin D3 to protect you from your environment. It’s time for many of you to scale your knowledge to the biophysical scale because this is how sunlight affects your protein polymers in your skin to scatter bad radiation and allow optimal absorption of the proper frequencies of sunlight by your blood and its cells.
CITES
1. Modern Actinotherapy. R. H. Beckett. 1955.
2. http://www.sciencedirect.com/science/article/pii/S1089860305001795
3. http://en.wikipedia.org/wiki/Rayleigh–Bénard_convection
4. http://en.wikipedia.org/wiki/Crabtree_effect
5. http://www1.lsbu.ac.uk/water/grotthuss.html
6. http://www.ncbi.nlm.nih.gov/pubmed/25325256
7. http://www.ncbi.nlm.nih.gov/pubmed/10759480
8. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3134326/
9. http://jp.physoc.org/content/early/2009/03/13/jphysiol.2008.167692.full.pdf
10. http://www.dvdres.com/content/5/2/82.full.pdf
11. Weinberg et al., Free Radic Biol Med. 46(12): 1626–1632, 2009
12. S. Hatse et al. “Vitamin D status in newly diagnosed breast cancer patients inversely correlates with tumor size and moderately correlates with outcome,” SABCS 2011; Abstract P5-05-01
13. http://www.ncbi.nlm.nih.gov/pubmed/12730293